Experiments with transdermal hormones
-
INTRO
I find using various hormones highly beneficial to my quality of life. Since most hormones have poor oral bio-availability, transdermal application is the next best option. However, transdermal hormone delivery is not without it's own problems. I personally have yet to find a solution that I'm happy with, and that's why I'm creating this thread. I did have a thread already on the Ray Peat Forum (RIP), but I'm banned there. Link
Exogenous hormones are finicky
Transdermal products applied on the skin suffer from one major problem: duration of action. This is also an issue with orally administered hormones, but at least applying on the skin is more efficient at boosting blood levels.
Anyways, skin penetration is hard to control, and even worse, it's difficult to maintain as well. Most of the solutions for topical TRT rely on blasting T levels as high as possible. That way, by the time the T levels dip, it's already time for the next dose (presumably 24 hours later).
Spikes in hormones are not good
I don't like this approach. I think stimulating androgen pathways this aggressively every day is not wise. I would be concerned with stressing the body and organs with rapid and excess growth and potential cardiac remodeling.
Not only that, but the conversion to estrogen is also a problem. Sure, the massive amounts of T and DHT can balance out the increased estrogen; however I don't think that it's only the ratio of androgens:estrogens that matters. The receptor theory is incomplete, and I figure that exposing the body to increased estrogens is not wise, even if there are enough androgens to prevent estrogenic symptoms.
Therefore, my ideal transdermal hormone mixture would not only maintain levels throughout the day, but it would also penetrate enough hormone for there to be an effect that could justify the hassle of using topical products.
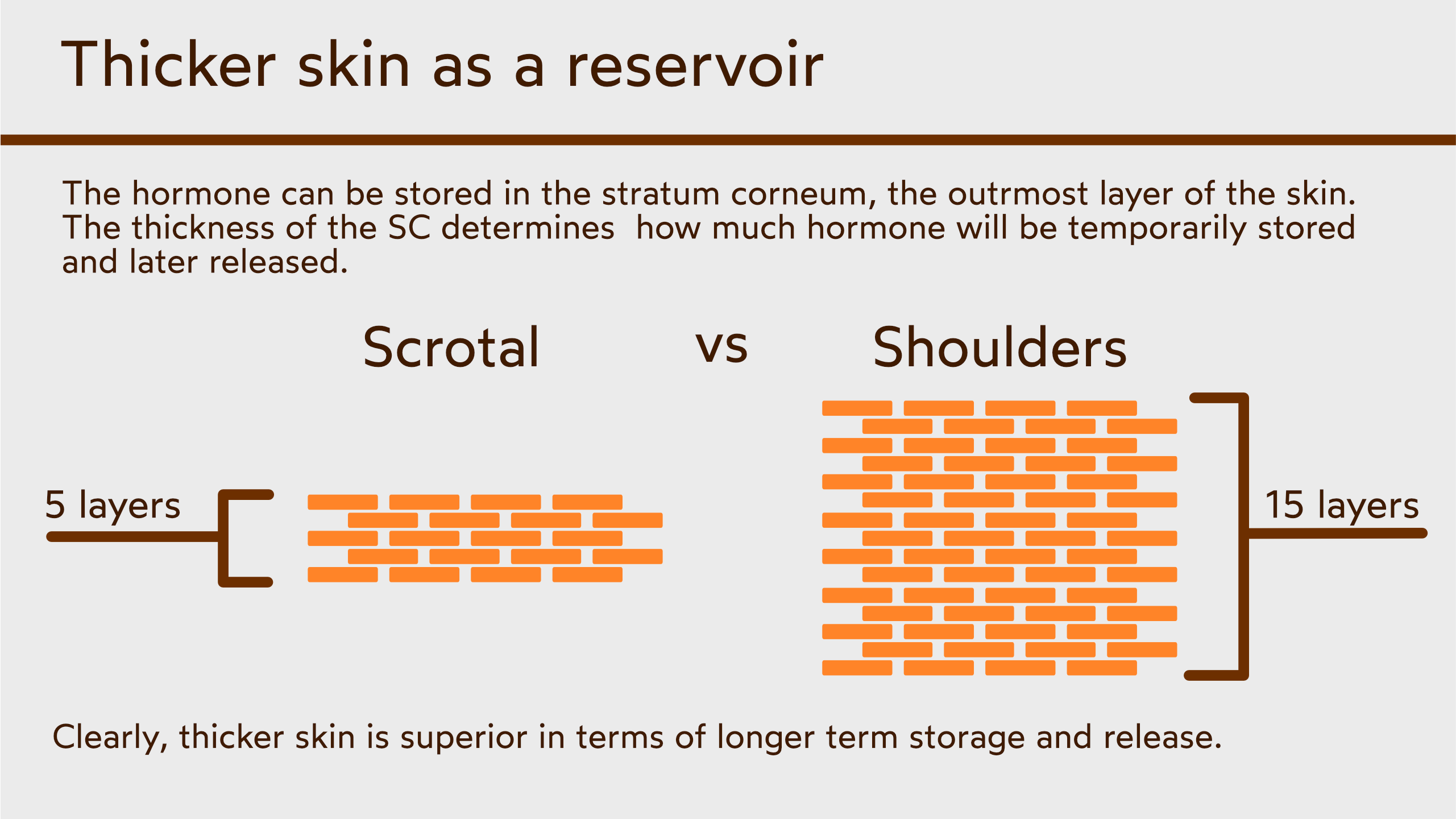
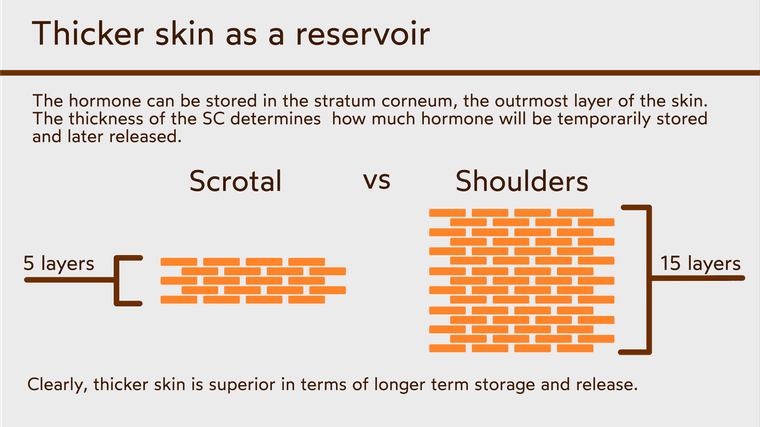
Problems of the different thicknesses of skin
The area where the mixture is applied also matters. For example, the scrotal skin is thin, and hormones can easily penetrate into the blood even without potent penetration enhancers. This means that by applying hormones on scrotal skin, you get the same effect as you would from using DMSO+hormone combo on any random patch of skin - you get a massive spike that doesn't sustain hormones for very long.
You could solve this by reducing the strength of your mixture, and instead apply it on a larger surface area. This way the hormones absorb slower, but because of the larger area, you would still get a steady dose to last the entire day. Except, this wouldn't really work, since scrotal skin has a very limited surface area.
Applying on thicker skin is the next option, somewhere like the shoulders is usually good. However, people typically say that it's too weak, and that also doesn't last the whole day. Fortunately, the surface area is much larger, and you can apply a lower % mixture with more penetration enhancers to maximize this methods advantages.
You can think of it like this. Absorbing huge amounts of hormones through thin skin with potent solvents like DMSO is like opening your kitchen faucet to max for a few seconds - you get a dump of water, but that quickly goes down the drain. On the other hand, absorbing hormones through thicker skin, over a larger surface area, at lower hormone %'s, with only medium penetration enhancers is like having 2 faucets open to a trickle. The amount of water that flowed through could be the same, but the rate that it flowed at, wasn't. At least that's the idea.
Problems of penetration enhancers
Anyways. Thicker skin poses a problem - lowered penetration. Things like DMSO and Benzyl Alcohol seemingly solve this. They both not only hold tons of hormone, but it also push a large amount through the skin with ease. The problem is that the most effective penetration enhancers are pretty volatile, and they dissipate quickly and their penetration enhancement goes away. Essentially, it becomes pointless to use this kind of mixture on thick skin, because the end result is pretty much the same as on thinner skin.
So an ideal penetration enhancer would not only be powerful enough to push a meaningful amount of hormone into the skin, but also hang around long enough for the hormone to leach into the blood stream through the day. I don't think this kind of penetration enhancer exists, since the nature of effective penetration enhancers is to be unstable. I think this problem is solvable, though.
For example, using a combination might work well. A powerful penetration enhancer to quickly drive lots of mixture into the skin, and then a weaker one to hang around for longer and provide a slower trickle. I've found menthol to be effective for this. It's quite powerful, but lasts longer in the skin than something like DMSO. And for the weaker penetration enhancer, perhaps something like lauric acid might work well. It's a moderately effective penetration enhancer, but since it's generally more stable, it should hang around for much longer.
Emulsion vs regular mixture
The next choice that I struggle with is the decision between an emulsion and a regular mixture. Emulsions carry a few benefits:
- they are easier to apply,
- they prolong the duration of the skin penetration,
- and they seem to be more powerful in my experience.
I've found that menthol in lotions feels cold at least twice as long in a lotion, compared to a simple liquid mixture. Lotions also seems to be all around more potent, probably because they contain surfactants (the emulsifiers). Additionally, the emulsified particles might penetrate into the skin a bit, but that's not super likely unless it's a microemulsion.
Lotions do have a few disadvantages too. They can mold if your preservatives are not very strong, and they can also separate over time. I personally haven't had such problems, but it's a possibility and highly depends on the lotion's ingredients. (terpenes like menthol, eucalyptol, and limonene seem to work very well as preservatives) Lotions also don't spread quite as thin as, for example, ethanol mixtures. I have hunch that lotions waste the most hormone on top of the skin. At the same time, this could be an advantage, since this left-over lotion would have a chance to absorb later in the day, while all evaporative-solvent based mixtures would dry up and leave the hormones in a solid form.
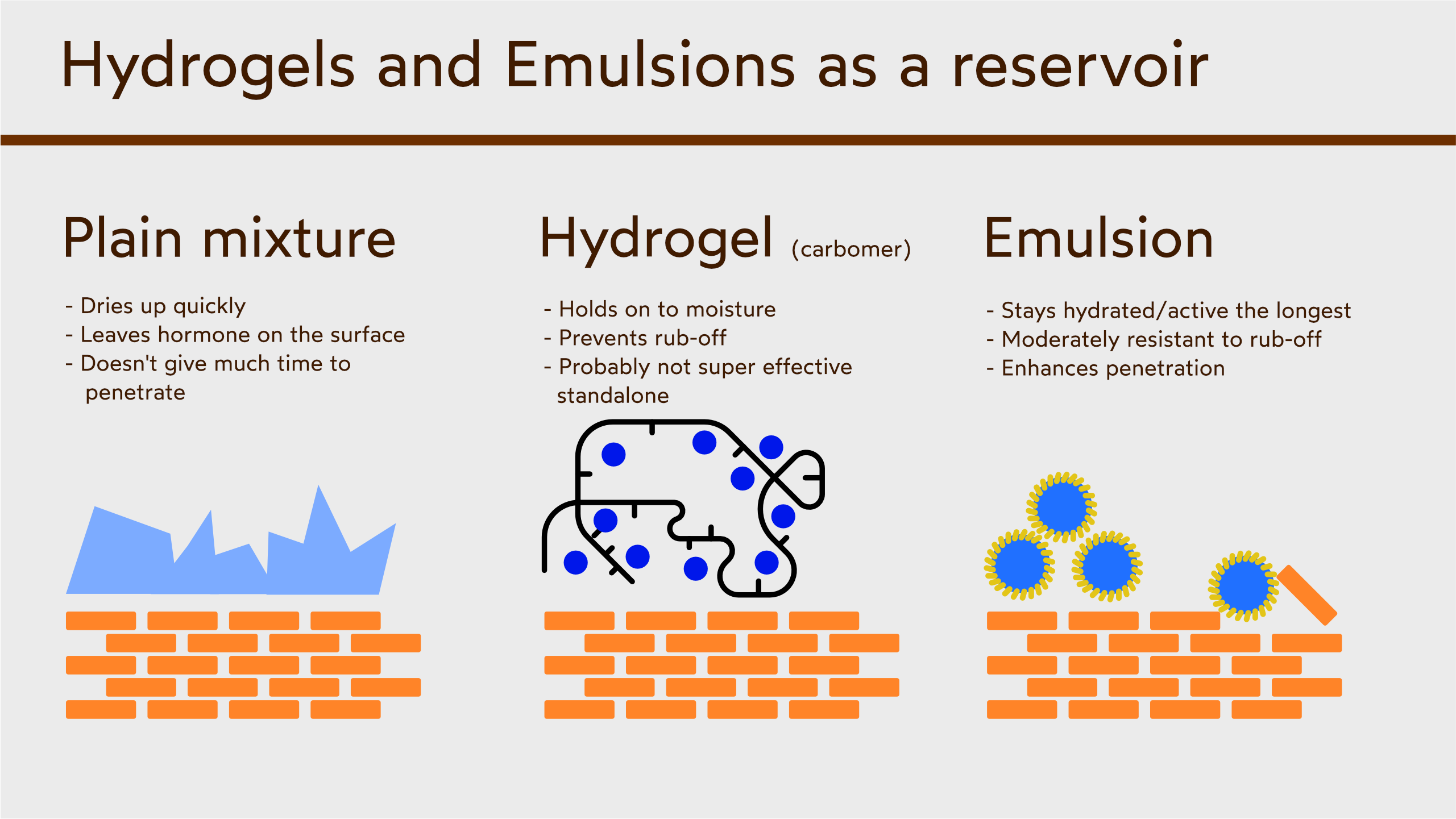
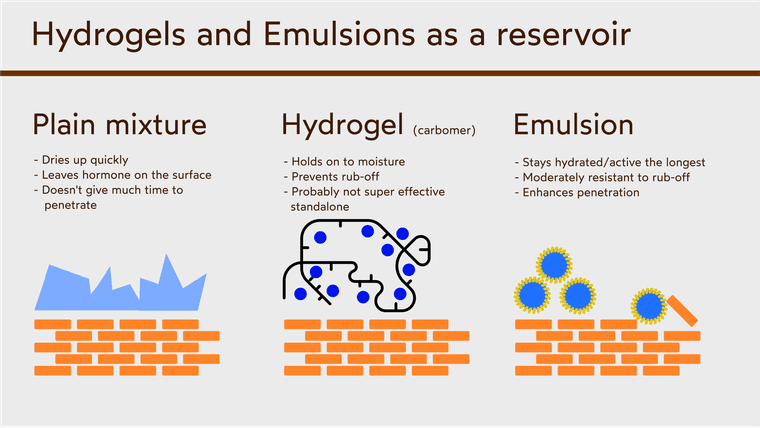
Reservoir
This brings me to the idea of a reservoir. Since it's so difficult to slow down absorption without reducing total absorbed hormone, creating a reservoir might work. The first idea is to store the hormone on top of the skin, like in a hydrogel or emulsion. This is probably not a super effective reservoir, since it will get rubbed off. I think that it could still be mildly effective providing a small increase in effectiveness. Something like an emulsion would work best, but combining it with carbomer might make it even more effective.
Next, you can use thick skin. As discussed before, the thicker skin will hold the hormone and leech it into the blood. Again, the trick with thicker skin is to use strong enough penetration enhancers to get it into the skin, but also not too strong so that they don't dissipate too quickly.
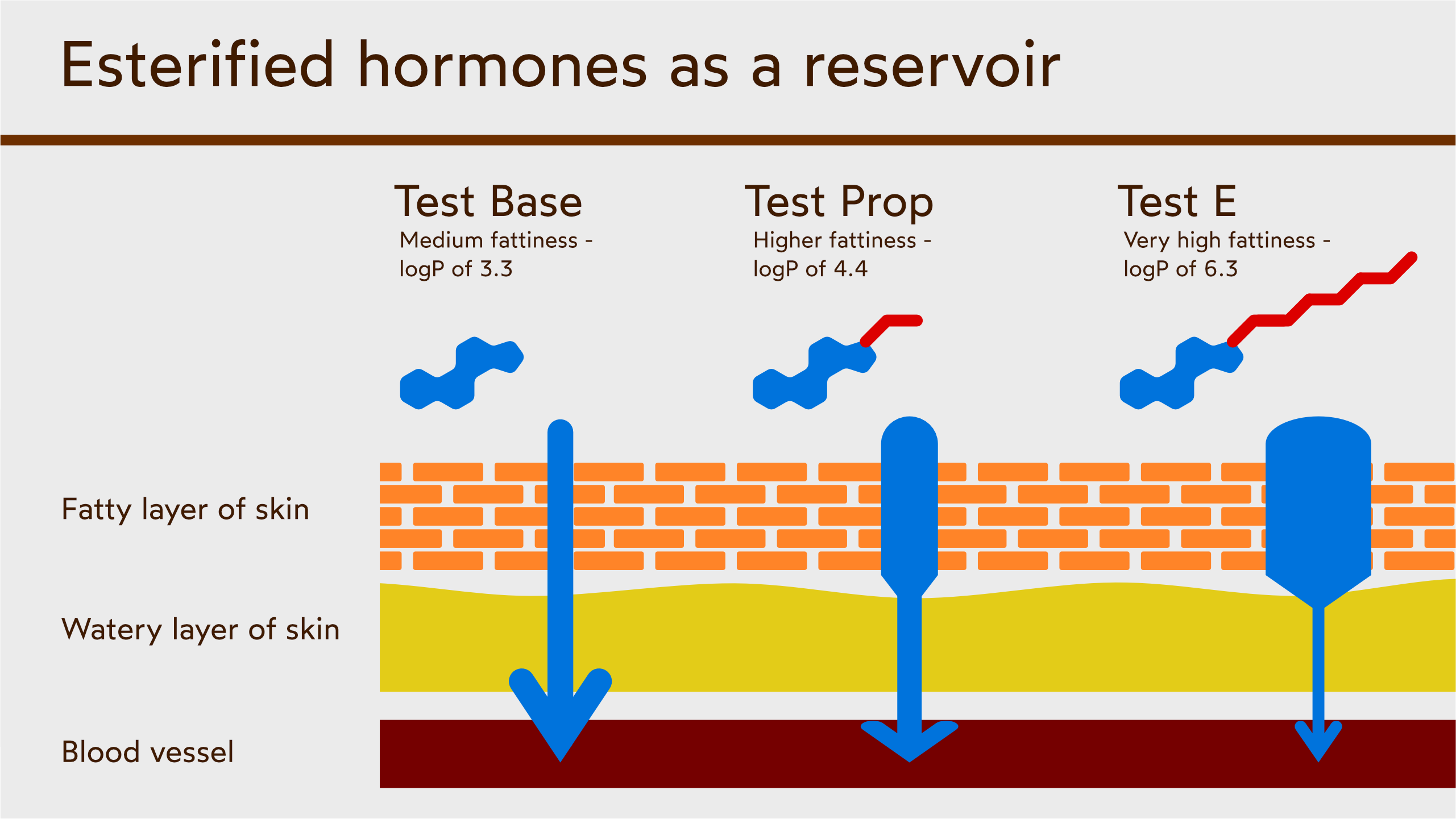
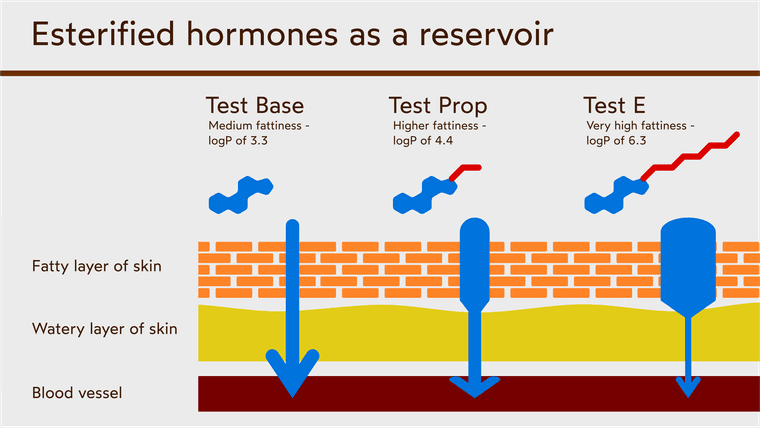
Lastly, using esterified hormones might work very well as a reservoir. Their increased fattiness means that they will absorb well into the more fatty stratum corneum, but not as well into the more aqueous deeper skin layers. This creates a bottleneck, and slows down the absorption into the blood. Since they are larger molecules, using extra penetration enhancers will be necessary, but the benefit of the bottleneck remains. Even with additional penetration enhancers, the esterified hormones will have a harder time crossing into the blood, and the bottleneck will still work well to damped the spike of hormone.
Plans for future experiments
I'm still debating on what kind of ingredients to use for future experiments. I have Mast P, which I think is close enough to Test to not really matter.
Menthol is reliable and an effective penetration enhancer. I also like propylene glycol as a non-volatile alcohol. It's a touch weaker than ethanol, but since it doesn't evaporate, it remains active for much longer.
Fatty acids are also good penetration enhancers. The longer chain ones hang around in the skin much longer, but naturally are much weaker. Lauric acid seems like a good middle ground, and isn't as smelly or hard to get as the really short ones like C8 and C10. Unfortunately, the fatty acids might become part of the emulsion interface, meaning they get incorporated into the wall of the "bubbles" instead of remaining inside. At the same time, the hormones can do this too, which might be a problem. On the other hand, I think that the emulsion might break upon contact with the skin fats, so perhaps this doesn't really matter.
Perhaps adding a low % of DMSO might be a good idea, mainly to quickly drive the solution into the skin and increase penetration enhancement via it's unique mechanism of protein denaturation. DMSO and ethanol also provide the benefit of increased spreadability and thinner application, increasing the efficiency.
At the same time, I'm not confident about mixing carbomer with DMSO, even at low dosages.
Another dilemma that I have is deciding upon a % for the hormone. Lower %'s mean you need to spread it across a larger surface area, which prolongs the effects but decreases the peak. Would combination of the reservoir techniques be enough to offset the peak, and allow me to use a high % of hormone? Or should I still aim for a low % to really stretch out that peak across the day?
If I use too low of a %, then application becomes a chore. Add to this the increased weight of the esters and it might be really bothersome to apply a few mLs of lotion to get a mediocre, albeit prolonged dose.
I'm not really sure what the balance is here, and to find out I'd have to run endless experiments which I don't have the time or interest in doing. Perhaps you guys have some fresh ideas, or new research that you stumbled upon?
-
@brightside Thanks for this thread.
-
What would be a good dose of topical T that would avoid shutdown
-
Depends where you apply, what's the solvent, how estrogen and androgen sensitive you are, how much cortisol you've got, how much body fat, etc.
A few mg's should be fine, but then you might not feel anything, so again, depends on all of the above.
-
Looking forward to this thread. I hope it gets the engagement it deserves.
I don't think people realise the profound health impact it can have if we and @brightside get a formula right...
Whats your opinion on a solution of 70% menthol , 20%DMSO and 10% Lauric Acid?
-
@brightside Do you think its possible to achieve a concentration of : 5mg test Per drop.
1mg dht Per drop.
1mg dhea Per drop.
1mg progesterone Per drop.
in a single solution?
This would be 100mg per ml of test and 20mg per ml of the rest.
-
 B brad moved this topic from The Junkyard on
B brad moved this topic from The Junkyard on
-
@brightside I moved this from the Junkyard to Bioenergetics Discussion since this thread seems better suited to that category. Let me know if you object and I'll move it back.
-
@metabolicmilk said in Experiments with transdermal hormones:
Looking forward to this thread. I hope it gets the engagement it deserves.
I don't think people realise the profound health impact it can have if we and @brightside get a formula right...
Thanks! If we could figure out a formula that's simple and cheap too, that would be great. Then people could use it to boost various hormones that people buy from haidut, for example.
Whats your opinion on a solution of 70% menthol , 20%DMSO and 10% Lauric Acid?
It would be really damn cold, lol. It would also be solid, since menthol and lauric acid are both solid at room temp.
Additionally, it might be irritating, but that depends. One time I made a lotion with nonanol and menthol which caused pretty substantial redness and irritation, even more than DMSO. Both ingredients by themselves were fine, but together, they potentiated each other's effects and were too disruptive to the cells. That might happen with DMSO+menthol, but perhaps not.
If I can incorporate DMSO into a lotion, then I think the above idea might work, since it being solid won't be an issue.
If you reduce the Menthol down to say, 20-30%, that should be fine. Also, are you talking about a solution that just liquid, or an emulsion? If it's just liquid you could just do - 30% Menthol, 20% DMSO, 10% LA, and then 10-20% hormone and the rest is just carrier liquid, either MCT or Ethanol.
I might try that once I get a refill of my DMSO, good idea.
-
@brad said in Experiments with transdermal hormones:
@brightside I moved this from the Junkyard to Bioenergetics Discussion since this thread seems better suited to that category. Let me know if you object and I'll move it back.
Thanks! No, that works for me. I just didn't know where it belonged
-
@metabolicmilk said in Experiments with transdermal hormones:
@brightside Do you think its possible to achieve a concentration of : 5mg test Per drop.
1mg dht Per drop.
1mg dhea Per drop.
1mg progesterone Per drop.
in a single solution?
This would be 100mg per ml of test and 20mg per ml of the rest.
Hmm. I'm gonna get a bit technical on you. (mostly because I've been meaning to bring this up in a thread somewhere)
Are we talking ethanol? DMSO? something else? Last time I measured, I got a different amount of drops from 1 mL of ethanol vs DMSO. Unfortunately, I don't remember the amount.
A different drop count per mL means different drops size/weight/volume, so your hormone concentration might not fit.
Also, I'm not sure if viscosity makes a difference on drop size. Say you have a solution that's 5% hormone vs 10% hormone. Would the drops change in size/weight or would the stay the same? The more concentrated solution is going to be more viscous, so theoretically it would mean a larger drop.
At the same time, I'm pretty sure it's the surface tension that actually matters. I do know that using different droppers will get you different sized drops. So a drop from a glass dropper will be bigger because ethanol can stick to glass, vs a plastic one it won't be able to stick to, so the drop will drop sooner and smaller. No idea how DMSO behaves.
This matters because if these factors do change, then you really don't know exactly how much hormone is in each drop. What if your mL gets stretched from 25 drops to 32, that means you wouldn't have 5mg T per drop, but only 3.9mg. If you plan to use a lot, then that adds up quickly. Your 100mg T dose would only be 78mg.
Would be cool if someone could chime in with some more understanding of this.
Anyways..
You would ultimately have to try it to see for yourself, but it does look like it would be a very tight fit. You're trying to fit 100mg(T) + 20mg(DHEA) + 20mg(P4) + 20mg(DHT) = 160mg of hormones into a milliliter of solvent that, at best, can hold 200mg/ml of DHEA, and at worst, 50mg/ml.
Also, do the hormones affect the solubility of other hormones? So for example, does the 20mg of DHT only "use up" 20mg/ml worth of DMSO, or do you need additional DMSO particles to stabilize it in solution, making it so that you actually use up more of the space that's supposed to be for other hormones.
That's just something else that I've been pondering on. It doesn't really answer your question though, lol
-
@brightside What's the reason for transdermal over injecting the hormones?
-
@jwayne said in Experiments with transdermal hormones:
@brightside What's the reason for transdermal over injecting the hormones?
Few reasons. For me, injection seems like a primitive method, while topical is a much more elegant solution. But the general reasons would be:
- risk of infection
- introducing needless PUFAs
- long term suppression and need for PCT to stop
- more of a commitment/big deal to do (buying potentially contaminated UGL gear or going to a TRT clinic)
- more often a need for AI (since topical generates more DHT)
Additionally, this is only for TRT, but people might want to use other hormones like P5, P4, DHEA, DHT, Exe, 5aDHP, etc. Using topically is convenient and can offer a high absorption compared to oral, or it can provide an alternate metabolism. (like in the case of DHEA or T).
I've purified some exemestane from some pills and used it topically. It worked well, and personally I would prefer to use a few drops of exemestane than take a pill with microcrystalline cellulose. Also, topical bypasses the first-pass effect which degrades a large amount of exemestane that already has a poor absorption rate. Topical > oral in this case.
Lastly, the reason I put so much effort into this is because I find this topic interesting.
-
@brightside Hey, what is your current formula that gives the most satisfying results? I mean especially for the testosterone.
I have tried several formulas including DMSO, Ethanol, IPM, Menthol etc. But I could not find anything that I could stick to long term or that it would give me the results I want.
I think the biggest problem for me is the spike in hormones. Thank you.
-
Hi @brightside
I actually tried this last night. It was possible in a solution of 80%DMSO. 20% Ethanol. Dissolved perfectly fine. I believe one drop from my bottle is 0.05ml. The amount of liquid was exactly 100ml.
-
@milkgains_bro Also curious about this
")
-
@brightside Good reasons
-
My son Red Button, you still work at Staples brah?
-
@metabolicmilk said in Experiments with transdermal hormones:
Hi @brightside
I actually tried this last night. It was possible in a solution of 80%DMSO. 20% Ethanol. Dissolved perfectly fine. I believe one drop from my bottle is 0.05ml. The amount of liquid was exactly 100ml.
Do you not absorb ethanol to the point of toxicity when it's mixed with DMSO ?
-
The amount of ethanol is very small. In this solution per application it will be only 0.05ml. ( 5 drops and ethanol is 20% of the solution ). I think even with DMSO potentiating effects it is negligible. I certainly don’t feel anything. The ethanol is there to clean the application area. I think the danger of potentially absorbing unwanted things due to the presence of DMSO is more of a risk than 0.05ml of ethanol. Haidut I believed used to use this ratio in his DMSO products and he is a much smarter man than me so if it’s good for him it’s good for me
-
I wonder what SFA esters Haidut uses? And where you'd even go to buy such things. Haven't seen that on Amazon.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login