Rosacea
-
What information is out there on improving or even curing rosacea?
There is this RP article on it: https://wiki.chadnet.org/rosacea-inflammation-and-aging-the-inefficiency-of-stress
He suggests it's due to a mitochondrial issue and shows how women with higher amounts of estrogen get rosacea more.
However, I have had rosacea for a long time, and even when I load up on androsterone (powerful AI) while taking pyrucet + niacinamide, all while not being a woman, it doesn't really go away. The only thing that's made it better is a special metronidazole cream from my dermatologist and I cannot find any info on that here or on RPF.
-
Have you tried topical niacinamide?
-
Try the topical red dicopperoxide. Or better yet, topical Cu(II)-(acetyl salicylate)2.
Association /= causation.
Estrogen is elevated to increase copper availability through enhanced ceruloplasmin synthesis and cellular copper uptake transporter. Women after menopause accumulate iron without being replete in copper to compensate for this wrt to their ferroportin 1 and superoxidedismutase etc.
In lab models rosacea is typically induced by administration of the antimicrobial peptide LL37. LL37 of course is a product of D3 isomerization to 1,25-OH-D3 and IFN-y to tackle infection or as a response to significant endoplasmic reticulum stress. Therefore it may just be a convenient but replacabe means for inducing local inflammation at the intracellular level.Anyhow it's amazing how much nonsense RP blasted out sometimes in a potpourri of the usual keywords and how he was all about the dangers of PUFA and iron and even in that linked article above mentioned that "it can spread the damage to other components of the mitochondria, including the cytochromes and the polyunsaturated fatty acids" but never once pointing to copper which is necessary to control the intracellular iron accumulation, the ferrophagy, the Fenton reaction, the resulting lipoxidation, the conversion to iron's safe and stable Fe3+, the folding and stabilization of the fatty acids for cytochrome c, control blood viscosity through keeping Factor VIII in check and last but not least of course the collagen and elastin crosslinking to maintain sufficiently thick and supple skin.
as for iron overload, impaired mitochondrial function, impaired cytochrome C and the mentioned functional oxygen deficiency enjoy:
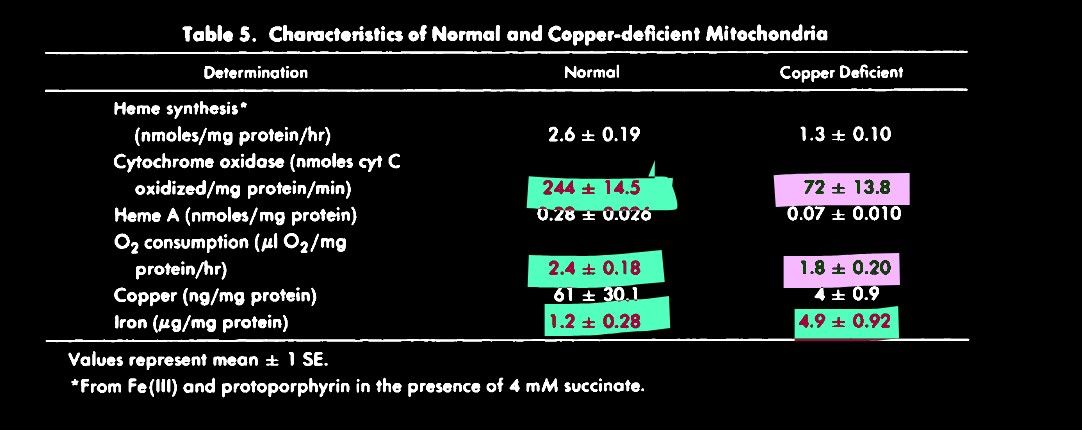
from https://ashpublications.org/blood/article-pdf/48/1/77/579793/77.pdf -
Have you tried activated charcoal? I’ve turned many people with skin issues on to it, and in my experience skin problems are almost always endotoxin.
When I first cured my own issues I used two tablespoons of charcoal in about 8oz of water after meals for two weeks. Now I just pop a few pills here and there if needed, but I’d consider myself cured.
-
I have very bad rosacea, looks like I am sunburnt all the time and the only thing that works for me is the medication Rhofade. I have only used it a few times though because of my fear of the “rebound effect”, plus I don’t even know if it is a safe medication to use from a holistic perspective. I don’t understand chemistry but it looks like it is an alpha 1 receptor agonist and vasoconstrictor.
Are there any Peaty vasoconstrictors out there?
My rosacea is the type that has been with me since a small child, I would flush with exercise, but in my adolescence it slowly became permanent until my face is red all the time. So different from the type of rosacea Peat discusses in his article on it, the type associated with alcoholics with the red hardened nose and visible blood vessels.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login