When you get a virus infection, it stops you making glycogen +effect of carbs w virus vs bacteria
-
https://academic.oup.com/jcem/article-abstract/69/2/317/2652052?login=false
The rate of glucose infusion required to maintain normoglycemia during hyperinsulinemia (∼500 pmol/ L)
During infection, the glucose requirements {for reaching a glucose level when high insulin} in the patients [21 ± 2 (±SE) μmol/kgmin] were 52% less than those in weight- and age-matched normal subjectsOne to 3 months after recovery, the patients' glucose requirements {to reach a glucose level after insulin} were still significantly lower (37 ± 3 μmol/kg.min; P < 0.02) than those in matched normal subjects.*
This decrease was due to a defect in glucose utilization (18 vs. 37 μmol/kg.min; P < 0.001, patients vs. normal subjects). Total carbohydrate oxidation rates were similar in both groups (16 ± 2 vs. 14 ± 1 μmol/kg.min, respectively), *whereas the apparent glucose storage was neglible in the patients (2 ± 1 μmol/kg.min) compared to that in normal subjects (22 ± 2 μmol/kg.min; P < 0.001).
So glycogen creation goes from 22 umol/kg/min to 2umol almost none with an infection.
any thoughts on that
--
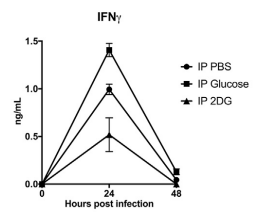
Infection -> muscle insulin receptors downregulate because of IFN-Y -> high insulin -> high insulin in blood triggers T cell activity https://www.cell.com/immunity/fulltext/S1074-7613(18)30241-3 (its the high insulin not high glucose)
starvation promotes lethality upon influenza infection of mice, which could be prevented by oral glucose gavage.
However, caloric supplementation during viral infection does not induce loss of glycemic control^ goes with the saying feed a cold starve a stomach bug. from what i remember you can wipe out 50% of some bacteria with a 24h fast (which is also on the edge of where it becomes significantly damaging to small intestine).
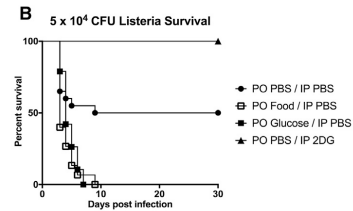
https://www.cell.com/cell/pdf/S0092-8674(16)30972-2.pdfFeeding bacterial infection with carbs = more death: (injecting i.p instead of orally also similar)
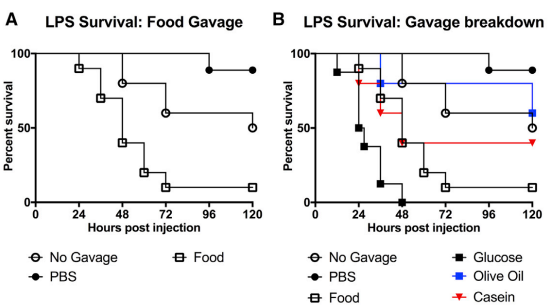
Just the LPS endotoxin, carbs worse too (not only a result of feeding bacteria) - olive oil only not much change good survival, mixed meal still worse (PBS outperformed no food for some reason?)
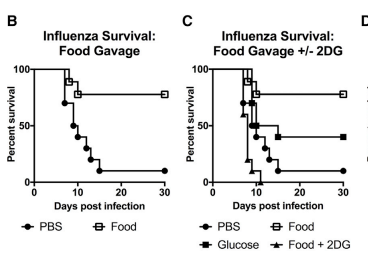
Instead with influenza , carbs = good survival (just virus not co infection
e.g if also had vomiting and diarrhea)
We observed that the administration of glucose to LPS challenged mice potentiated seizures, Together, these data suggest that the enhanced lethality caused by glucose supplementation in endotoxemia is likely mediated through increased ROS and neuronal dysfunction.
We next asked whether viral infections, which induce a different type of immune response compared to bacterial infections, were also affected by caloric supplementation.Caloric supplementation with
casein and olive oil provided little to no survival benefitwe found that gavage of 1 kilocalorie BID of enteral nutrition starting 8 hr post-infection protected mice from influenza-associated mortality (Figure 3B). Gavage of isocaloric isovolumetric glucose partially recapitulated the effect of enteral nutrition, whereas i.p. injection of 2DG {inhibits glycolysis} concurrently with feeding completely ablated the survival benefit
Viral load and inflammation not much different - the glucose helped lower ER stress & apoptosis
Whereas PPARa deficiency was lethal following LPS challenge, it was protective in influenza infection in a manner independent of pathogen control. This protective effect was not observed in FGF21-deficient animals
whereas impairment of ketogenesis, whether through genetic deletion of PPARa or glucose administration, was lethal in bacterial inflammation, it was protective in viral inflammation, in a manner independent of the magnitude of inflammation.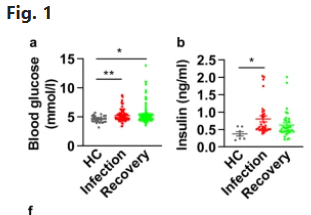
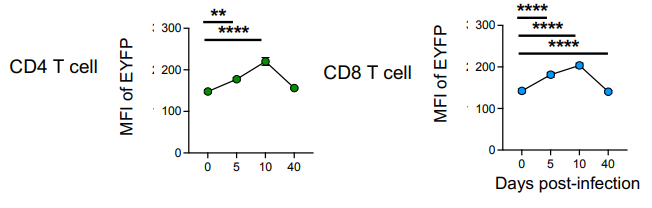
^ blood glucose in the non severe infections pretty much stays normal for most non IR people with the insulin increase. severe cases got elevated blood glucose too. but most people (majority of these were non severe infections) had elevated insulin and non significantly in recovery phase (2 days without a positive virus test) (covid) https://www.nature.com/articles/s41392-021-00822-xNotably, the numbers of total NK cells and NKT cells dropped substantially by day 10 and were slightly lower than in naïve animals. The numbers of Ifnγ+ T cells peaked at day 10 post-infection with similar numbers of cytokine+ CD4 and CD8 T cells. At day 40, their numbers remained above those in naïve animals
https://academic.oup.com/discovimmunology/article/2/1/kyad014/7246320?login=false
In mice IFN-Y peaks day 10 (even though virus peaks days before this and likely well cleared already by then)
https://www.science.org/doi/10.1126/sciadv.adi9379 humanscurious if its net beneficial, because it makes you less resilient to a following bacterial infection
https://www.semanticscholar.org/paper/Inhibition-of-pulmonary-antibacterial-defense-by-Sun-Metzger/5eb191cf376646f829396b3dfa45b9f1bd9624dfpulmonary interferon-γ (IFN-γ) produced during T cell responses to influenza infection in mice inhibits initial bacterial clearance from the lung by alveolar macrophages, and suppresses innate protection against extracellular bacterial pathogens in the lung.
This suppression of phagocytosis correlates with lung IFN-γ abundance, but not viral burden, and leads to enhanced susceptibility to secondary pneumococcal infection, which can be prevented by IFN-γ neutralization after influenza infection.
Direct inoculation of IFN-γ can mimic influenza infection and downregulate the expression of the class A scavenger receptor MARCO on alveolar macrophages -
@cs3000 can u give a tl;dr
-
Probably because the cells utilize more sugar as a concerted effort to recover from infection. If we picture a U curve, with the state of infection being one extreme side, more sugar would perhaps satiate the need to recover from infection with the surplus leveling out for glycogen formation.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login