Is Caloric Deficit Peaty?
-
I dont understand a lot of Peat Lit yet, bear with me.
Caloric deficit is useful for fat loss, but if you have caloric deficit by the end of the day, your body percieve you are in a state of starvation (low blood sugar) and release cortisol.
Is it different if the fats released are saturated rather than PUFAs?
Please help me understand! -
@highseabasch
depends. A calorie deficit can be put to good use if done wisely. Supplementing calories from sugar and eliminating PUFA should certainly help minimize the negative effect of the deficit on the hormonal balance. -
Not trying to sound like a CICOtard but you need a calorie deficit to lose weight/fat. Obviously other factors are important too (metabolic rate, macro and micronutrients, etc) but a calorie deficit is an essential factor.
-
“The larger the quantity of “toxic fat” stored in the body, the more careful the person must be about increasing metabolic and physical activity. Using more vitamin E, short-chain saturated fats, and other anti-lipid-peroxidation agents is important.”
“But when tissues contain large amounts of polyunsaturated fats, every episode of fatigue and prolonged excitation leaves a residue of oxidative damage, and the adaptive mechanisms become progressively less effective.”
“It’s the stored PUFA, released by stress or hunger, that slow metabolism. Niacinamide helps to lower free fatty acids, and good nutrition will allow the liver to slowly detoxify the PUFA, if it isn’t being flooded with large amounts of them. A small amount of coconut oil with each meal will increase the ability to oxidize fat, by momentarily stopping the antithyroid effect of the PUFA. Aspirin is another thing that reduces the stress-related increase of free fatty acids, stimulating metabolism. Taking a thyroid supplement is reasonable until the ratio of saturated fats to PUFA is about 2 to 1.”
“People with a significant amount of fat in their body, who have in the past eaten foods containing vegetable oils, are likely to draw unsaturated fats out of storage, with toxic effects unless vitamin E, thyroid, and coconut oil are used protectively until tissue stores of unsaturated fats are depleted. Typically, body stores of fat take four years to completely reflect the change to a different type of dietary fat.”
"When the diet has chronically contained more polyunsaturated fats than can be oxidized immediately or detoxified by the liver, the fat stores will contain a disproportionate amount of them, since fat cells preferentially oxidize saturated fats for their own energy, and the greater water solubility of the PUFA causes them to be preferentially released into the bloodstream during stress."
"In good health, especially in children, the stress hormones are produced only in the amount needed, because of negative feedback from the free saturated fatty acids, which inhibit the production of adrenalin and adrenal steroids, and eating protein and carbohydrate will quickly end the stress. But when the fat stores contain mainly PUFA, the free fatty acids in the serum will be mostly linoleic acid and arachidonic acid, and smaller amounts of other unsaturated fatty acids. These PUFA stimulate the stress hormones, ACTH, cortisol, adrenaline, glucagon, and prolactin, which increase lipolysis, producing more fatty acids in a vicious circle. In the relative absence of PUFA, the stress reaction is self limiting, but under the influence of PUFA, the stress response becomes self-amplifying."
-
When consumed, PUFA are preferentially stored whereas SFA/ MUFA are preferentially oxidised to provide energy. In context of a typically modern diet this would mean that the fat stores of most people will consist of predominantly PUFA. There have be recent studies to suggest that when fats are liberated through lipolysis (e.g. in a starved state), PUFA is preferentially released, which carries with it inflammatory and anti-metabolic activities. Whether PUFA is preferentially released due to a high concentration in the fat stores of most people or whether it’s due to another mechanism idk. @haidut talked about these studies on RPF. Generally Ray advocated for slow re-comp instead of caloric restriction, which is made more effective by the pro-hormonal effects of he’s dietary & metabolic recommendations. But he did recommend a person to take Vitamin E when dieting to protect themselves from the effects of FFA.
-
@Alexander99 Optimizing metabolism is more important than a calorie deficit. Eating sugar is NOT what this means. Glucose is the fuel; optimizing metabolism is providing the things to optimize the burn (=oxidative metabolism=citric acid cycle=Krebs cycle). Two important items are good thyroid function and having enough thiamine, but there are other things too.
for example:
I packed on 25 pounds in 25 days after taking Bactrim antibiotic which blocked my thiamine function. Although I resolved my thiamine issue via high dose thiamine hcl, I did not lose the weight until I changed the way I took my niacinamide (from taking 200mg, 2Xday to taking 100mg, 4Xday). When I changed the niacinamide supplementation, I lost 35 pounds in about 6-8 weeks. My diet remained constant. -
@TexugoDoMel In short, burning fat in small intervals is OK unless the fat stores contain PUFA, which damage cell function and release cortisol etc?
-
@mostlylurking Totally agree, I'm not sure if my post was poorly worded but I did not intend to contradict this. I was in the position years ago (before Peat and metabolism came into my cognitive awareness) where on 1500 calories a day I was not losing weight (or if I was a large deal was muscle mass). Obviously, the issue there was metabolism, not that I wasn't cutting hard enough.
I'm in the middle of a cut now and my priority is monitoring my metabolic rate through keeping an eye on temp and HR, not calorie counting. My point in the above post was more that you should have a calorie deficit when losing weight, but this is one, albeit an important one, of many factors in losing fat.
-
I think it's better to lose fat slowly so as not to overload the body with PUFA. Peat says that using aspirin, niacinamide, vitamin E, coconut oil, is welcome because it provides support and stability for safer elimination (glucuronidation), anything considered "prometabolic" can help with this. So if you're going to opt for a "forced deficit" by reducing calories, don't do anything crazy.
In my mind, if you're not obese, it's better to choose to create a deficit by increasing your metabolism than to force a violent deficit by reducing your needs too abruptly.
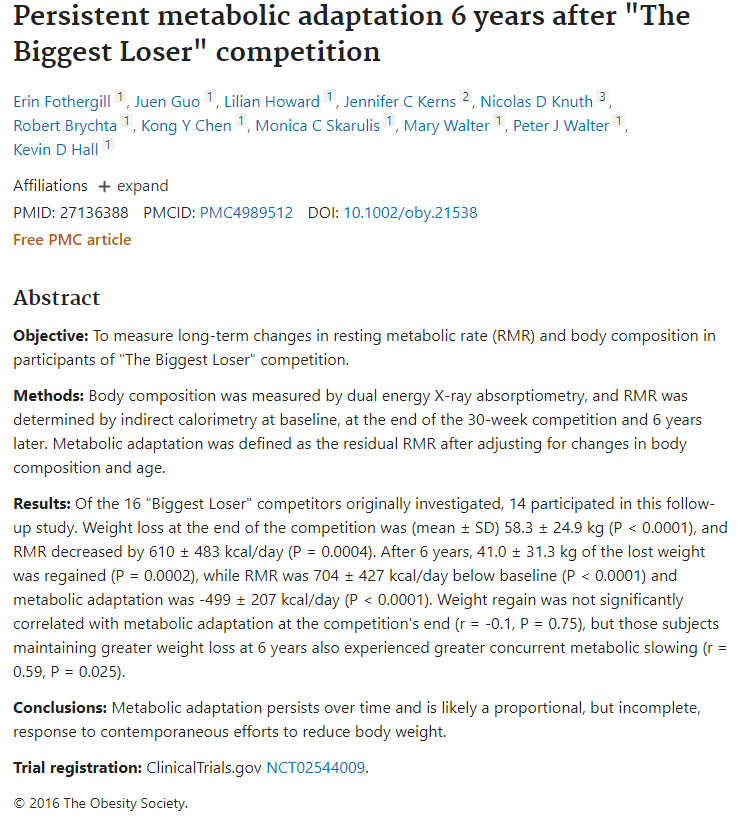
Here's an example, a short period of drastic deficit and the metabolism was depressed for 6 years.:
"After 6 years, 41.0 ± 31.3 kg of the lost weight was regained (P = 0.0002), while RMR was 704 ± 427 kcal/day below baseline (P < 0.0001) and metabolic adaptation was -499 ± 207 kcal/day (P < 0.0001)."
-
@Alexander99 said in Is Caloric Deficit Peaty?:
My point in the above post was more that you should have a calorie deficit when losing weight, but this is one, albeit an important one, of many factors in losing fat.
The trouble with the idea of a "calorie deficit" is just how exactly do you figure out what that means for you? If you have dieted using calorie deficits in the past, your body can reset its metabolic rate so that you can withstand calorie deficit (=starvation/deprivation) better which means you would need to reduce the calories even further to get any weight loss. This also opens the way to lose muscle mass (from higher cortisol) instead of losing fat.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login