Thiamine and Magnesium timing
-
I was looking to start taking Thiamine (TTFD) paired with Mg Glycinate and a B complex. I have read the thiamine will be mentally stimulating so people like to take it earlier in the day, but I usually take the Mg in the evening to sleep. Do they have to be taken at the same time? What else should I know when I start supplementing these? Thank you
-
I suppose it's for optimizing the energy level. If it's for another purpose (brain), it doesn't change the recommendations, as it's supposed to enhance a better carburation.
Thiamine before breakfast and lunch, preferably 15' before the meal.
=> Energy requires B1 B2 B3, especially B1. Not only.
You're going to burn more B2 if you take HD B1. Not necessarily every day for B2.Figure: See the circle "Citric acid cycle"
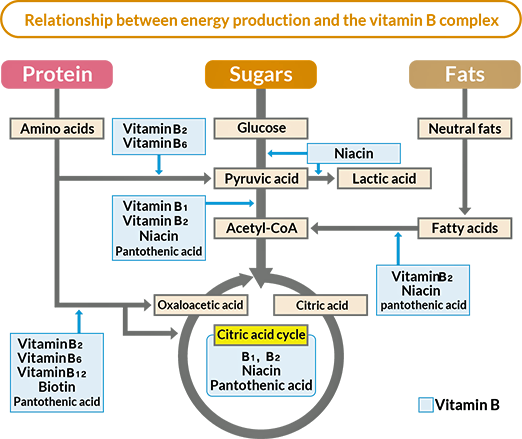
2 steps
*) Step one: Carbs / glucose => Pyruvic acid => Acetyl CoA
Vitamins B to produce pyruvic acid and acetyl CoA
https://pmc.ncbi.nlm.nih.gov/articles/PMC7019700/
Which vitamin converts glucose to pyruvate?
=> B3 (NAD)
Which vitamins convert pyruvate to acetyl CoA?
=> B1 B2 (FAD) B3 B5 (pantothenic acid)
Briefly, macronutrients are oxidized (step one) into acetyl-CoA through several pathways including glycolysis, which produces pyruvate from glucose, and vitamins B1, B2, B3, B5 and C play important roles.
*) Step two: Acetyl CoA => Citric Acid Circle (Krebs circle)
Which vitamins are required to pass through Acetyl CoA to Citric Acid Circle?
=> B1 B2 B3 B5.
=> + other B vitamins (B6 B8 B12) and Fe Mg
Then acetyl-CoA enters the citric acid cycle (step two), which generates energy as NADH and FADH2 through a series of eight oxidations that involve vitamins B1, B2, B3, B5, B6, B8 and B12 as well as iron and magnesium.
*) Step three: Energy production
Finally, the electrons of NADH and FADH2 are transferred to the electron transport chain (step 3), where they provide energy used to generate ATP molecules; this step needs the input of vitamins B2, B3, B5 and of iron.
Source: https://pmc.ncbi.nlm.nih.gov/articles/PMC7019700/
Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. 2020 doi: 10.3390/nu12010228If I try to summarize:
Energy metabolism in two steps
Step 1 is the catabolic breakdown of carbs, fat, and protein to extract energy in the form of electrons.
Step 2 is the translation of that energy into ATP using oxygen.*) Energy and nutrients needed for metabolism
- Carbs => Pyruvic acid => Acetyl CoA: Mg, B1 B2 (FAD) B3 (NAD) + B5
Required nutrients to extract energy in the form of electrons (electrons in the transport chain) (= oxidative phosphorylation => oxidation-reduction reactions are vital for ATP synthesis) - Acetyl CoA => Citric Acid Circle (Krebs circle): B1, B2 (FAD), B3 (NAD), Mg, Mn, Fe, GSH + B5
https://coremedscience.com/blogs/wellness/what-vitamins-give-you-energy
https://www.nature.com/scitable/topicpage/nutrient-utilization-in-humans-metabolism-pathways-14234029/
Note1: If you take a high dose (HD) of one element, you may encounter problems elsewhere. Here HD B1 => Some B2 required. Otherwise it would be as if you were lacking B2 (exhausted).
Note 2:
Proportions of vitamins B
- the same quantity of vit B1, B2 and B6.
- at least 4 x more vit B3
- at least 2 x more vit B5
Source : Zoelho.com (in French) Pharma-Dr.
Pay attention:
*)Some people feels nervous when taking high dose of B6 Pyridoxine (PNP). Unbalanced nervous system. DA 2 – 3 mg B6. Orthomolecular pharmacology 10 – 50 mg.
*)Feels better with Benfotiamine or Thiamine HCL than with TTFD (thiamin tetrahydrofurfuryl disulfide). TTFD passes the BBB.
*) B3. The form to privilege is niacinamide
Niacin has different names
Niacin = generic name
Nicotinic acid = pyridine-3-carboxylic acid.
Nicotinamide = niacinamide or pyridine-3-carboxamide
Other derivatives: e.g. nicotinamide ribosideKeep in mind: You’re artificially changing the system by adding extra dose of something, without taking into account the possible side-effects. But if you can listen to your body, why not if you want to experiment …
- Carbs => Pyruvic acid => Acetyl CoA: Mg, B1 B2 (FAD) B3 (NAD) + B5
-
@jakeseeds said in Thiamine and Magnesium timing:
I was looking to start taking Thiamine (TTFD) paired with Mg Glycinate and a B complex.
I won't take a B50 complex every day. I take 2x/wk.
As you didn't tell much about your purpose / problem, I'm not going to develop. -
@LucH Ok thank you! Yes main purpose is energy and brain function so I'd assume they go together? Thank you for the explanation, yes I am supplementing without taking into account possible side effects as I am just listening to my body. An experiment if you will. So when would you advise taking the Mg, am I fine taking the B1 and B complex in the first part of the day and Mg after dinner?
-
@jakeseeds said in Thiamine and Magnesium timing:
So when would you advise taking the Mg,
I take magnesium bisglycinate, the one I prefer (glycine, Gaba-like effect). High effectiveness. Choose a powder that mixes well (dilution). Not HSN. mine comes from nutrixeal.com (French site).
Against stress, it's no use to take Mg before a stressful event.
I take it after. 300 mg Mg element is advised then. +/ 16% => 2 g powder. High bioavailable. See the chart.
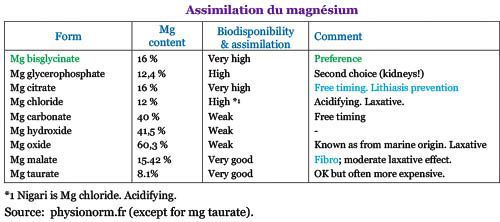
This kind of magnesium is best absorbed with food but I take it whenever I want / if necessary.
We need 4200 Mg element. Must be in balance with other nutrients: K/Na and Ca/Mg ratio.
It is often advised to take 2 x 300 mg Mg element /day. 3x/day if stress or anxious. In cure.
NB: 300 mg Mg element = 4800 mg powder of Mg bisglycinate (it contains 16% Mg element).
Exception: If your level vitamin D3 is too low (under 45 ng), do not take a high dose Mg on a regular base. Only punctually.
Personally, on a regular base, I check with my diet-software to approach 4500 mg/day.
between 1.25 and 2 g powder 2x/d according to what I've eaten. Often 2 g.
You can take Mg with vitamin B.For other comment about B1. Tomorrow. Too late here.
-
About High dose thiamine (HDT)
I know we have to reach 1500 mg B1 to see some neuro-improvements (through the vagus nerve).
But it's not advised to do it without staples (every 10 days), with 200-300 mg takes.
Of course, according to your feeling, the staple can be prolonged. Or perhaps you'll have to go back to 2 former staples whenever you feel "disconnected" / upset. Overton advises to stop the supplementation completely before taking it again, at the beginning of the process.Take Dr Allil overton and Chandler Marrs as references. Details on next post
Excerpt from the video of Allil Overton
1.23.16” Effective dose for different forms of thiamine
Type of vitamin effective amount
Thiamine HCL 500 – 4000 mg / day
Benfotiamine 300 – 1800 mg / day
TTFD 100 – 1500 mg / day
*) 1.26.21””: Paradoxical reaction: Temporary worsening of symptoms (from left to right side)
Don’t begin with a high transition (from 500 to 2 000 mg B1) because 80 % people will feel horrible.
People who’ve been deficient since a long time (10 years or more without taking a supplement and eating refined carbs with pasta, bread and / or rice) are more susceptible to encounter body reactions. Idem if you suffer from a chronicle disease (since B1 has been exhausted or in a very limited amount to assure all neuronal tasks). So open a 500 mg capsule and start with a portion of the powder, if required, and don’t jump to 2 000 mg at once. Begin very low and start very slow: Make transition (baseline on the graph). Only raise the dose when the baseline brings an improvement in symptoms and consolidate before raising again. Of course, we don’t raise the dose if someone feel worse; otherwise it’s going to make the situation 10 times worse. We stop taking B1 until we recover. We must be then patient and begin again with a very low dose, before building up very progressively.Synopsis of the video on next post
-
The Art and Science of Mega-Dose Thiamine Lecture: Part 1
EONutrition – Elliot Overton (nutritionist) – Video 1:34:21
This is the first of two lectures I gave to a group of medical/health professionals on the clinical application of high-dose vitamin B1. In this video I outline the basics of how the body uses this nutrient, why deficiency is likely more prevalent than it is conventionally thought to be, and how high doses may be working via different mechanisms to improve chronic health issues.
https://www.youtube.com/watch?v=-Uf1D2KdTn0
HDT = High Dose Thiamine
Synopsis (with time-code)
*) Video 5.55’’: The system affected by thiamine deficiency
*) +/ 6.00”: Symptoms of beriberi
*) 11.00”: Prevalence of B1 deficiencies (by ordinary people)
*) 12.30”: Medical dogma (incorrect)
Deficiency easily detected by blood test.
*) 14.00”: Common causes of deficiencies (classical risk factors)
*) 15.00”: Most tests are inaccurate
*) 22.00”: You’re out of the box (optimal status)
*) 23.45”: Hormones matters (reference site)
*) 24.25”: Everybody consuming high carbs will suffer from thiamin insufficiency. But not only.
See Figure.
Mind refined foods, inflammation or infection, environmental toxicity, surgery, etc. It increases the demand or it counteracts the enzymatic system. It increases the demand above the board (> 70%).
A appropriate diet is going to sustain you well but – surrounded by so many stresses – to rely on diet solely is not enough / inappropriate.
Many people can’t recover from a pathology because some medications impact the assimilation or the biodisponibility of vitamins.
*) 29.15”” The status of thiamin depends on the level of carbs eaten, even if not refined. High intake of macronutrients in the absence of micronutrients leads to health problems.
*) 30.00”: Recap
*) +/ 31.00”: Metabolic pathway of energy
If you haven’t enough vitamin (TPP, in blue = B1), you can’t use enzymes (yellow).
*) 32.00”: Same evidence: TPP (B1) is needed for carburation.
Figure.
TTP is needed by enzymes required in cellular energy. A continual supply must be brought. Thiamin is a rate-liming factor for energy production: With insufficient B1, the enzymes are effectively blocked and the entire process of energy production slows down. This is central in the process energy at practically at all energy level of the cells (mitochondria).
*) 32.55”: Krebs cycle.
Another figure to represent glycolysis
*) 33.05”: TCA cycle – Without enough thiamin, pyruvate spills into lactate (acidosis).
*) +/ 35.00” Enzyme pathway with B1
*) 35.45””: Thiamin is dependent on magnesium (activation), like many vitamins.
*) 39.05” Vagus nerve. Pathway involved in vagus nerve stimulation. Link with most visceral organs.
*) 39.30” – 44.20” Cholinergic anti-inflammatory pathway
Figure.
Several studies show that the decrease in cholinergic neuron activity correlates with the degree of severity of many neuron pathologies. It inhibits the release of pro-inflammatory cytokines. So, choline indirectly plays a role of modulator against inflammation. The vagus nerve is well the most determinant communicant factor in immune response.
If you lose the ability to communicate the signal from the brain through the vagus nerve, it will take an eternity to recover. Consider too that there is a two-ways communication. Without effective communication between sympatric and para-sympatric brain, we lose the ability to modulate an adaptive response. The system controls itself through the vagus nerve.
*) 44.20” Thiamine, a universal stress molecule.
Extra high thiamine levels protect the cell against injury (upregulation of recovery process), inflammation and oxygen stress.
*) 50.00” The effect of hypoxia on the brain due to a lack of thiamin cofactor
Figure with Krebs cycle and enzymes sensitive to B1 deficiency: TPP & ketoglutarate dehydrogenase.
=> Damage to neurons & mitochondrial dysfunction (reduced ATP production and oxidative stress).
*) 55.00” Book
*) 1.03” Recap
*) 1.04” References
*) 1.14” Enzyme Inhibitors (KGDHC inactivation) lead to problems
KGDHC = α-ketoglutarate dehydrogenase complex (mitochondrial enzyme depending on thiamine)
*) 1.15.45” figure. Thiamine chemistry is disrupted by environmental stress
*) 1.16.55” Figure. Enzyme inhibition
*) 1.1845””. Figure. High dose nutrient therapy
If you saturate the cell with a huge amount of thiamin, it doesn’t account (no problem). You’ll speed the process up.
*) 1.21.45: blood test and company
*) 1.23.16” Effective dose for different forms of thiamine
Type of vitamin effective amount
Thiamine HCL 500 – 4000 mg / day
Benfotiamine 300 – 1800 mg / day
TTFD 100 – 1500 mg / day
*) 1.26.21””: Paradoxical reaction: Temporary worsening of symptoms (from left to right side)
Don’t begin with a high transition (from 500 to 2 000 mg B1) because 80 % people will feel horrible.
People who’ve been deficient since a long time (10 years or more without taking a supplement and eating refined carbs with pasta, bread and / or rice) are more susceptible to encounter body reactions. Idem if you suffer from a chronicle disease (since B1 has been exhausted or in a very limited amount to assure all neuronal tasks). So open a 500 mg capsule and start with a portion of the powder, if required, and don’t jump to 2 000 mg at once. Begin very low and start very slow: Make transition (baseline on the graph). Only raise the dose when the baseline brings an improvement in symptoms and consolidate before raising again. Of course, we don’t raise the dose if someone feel worse; otherwise it’s going to make the situation 10 times worse. We stop taking B1 until we recover. We must be then patient and begin again with a very low dose, before building up very progressively.
*) 1.29.25”: Thiamine nutritional interactions
*) 1.30.25”: How to deal with HDT
Preferably high bioavailability of Thiamine (TTFD). A b-complex will be needed. Potassium and magnesium too. Mg is very important, especially to avoid the paradoxical effect. 1 000 to 2 000 mg more potassium could be helpful too (or coconut water if you don’t want to).
Note 1: If problem with TTFD (neuronal exacerbation), take another form.
Note 2: Do not take a B-50 complex alone every day (cell overgrowth stimulation)
*) 1.32.55’ Info (book):
Mega-Dose Thiamine – Beyond addressing deficiency. Elliot OVERTON
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login