Everything about high blood pressure
-
Please share everything you know about high (and low) blood pressure
-
hey man
-
Good day Ms Paddington.
Obviously the vasculature is a vast subject to try and trivialise. And obviously any attempt from me is going to be bent for fluid balance and dynamics.
Meanwhile @Amazoniac, @Peatly and @LLight (should they arrive) blew my mind on a regular basis on these subjects in the bad place. Hopefully they also have something to add. As does your intellect with a side of heart.
Obviously it is also Friday night. Therefore I will be back tomorrow.
-
For low blood pressure what helped me was increasing salt. When it comes to high blood pressure I am clueless. I can tell you lots about what Dr. Peat has written or said about it but I’m sure you can find that information and interpret it better than I could. What causes high blood pressure varies for each person and solutions will vary accordingly.
Ray Peat on High Blood Pressure
This thread is related
-
Paddington. It will take a little while for me to get my brain to play ball on this. But I and it will.
I'd like to say something useful about where volume status and blood pressure intersect. For is "high blood pressure" really high blood pressure, if the patient has issues with volume status.
-
@ursidae said in Everything about high blood pressure:
hey man
Hi, ursidae. I hope that you're well.
One interesting piece that I have to share is this:
Contributions of Sodium and Chloride to NaCl-Induced Hypertension
"[..]a limited number of clinical observations also indicate that blood pressure is not increased in humans by high dietary sodium intakes in the absence of chloride. In 1929, Berghoff et al reported that blood pressure increased in 7 hypertensive individuals on a high NaCl intake, but not on a high sodium bicarbonate intake.[2] This observation was subsequently confirmed.[3] Similarly, other investigators have also observed that in contrast to the increase of blood pressure induced by a high NaCl intake in hypertensive patients, blood pressure is not increased by a high sodium intake provided as sodium phosphate or sodium citrate.[1] Further suggesting a modulating effect of dietary chloride on blood pressure, in hypertensive and normotensive subjects, substitution of dietary NaCl with equimolar sodium bicarbonate leads to a reduction of blood pressure.[4,5] Additionally, in hypertensive humans, the reduction of blood pressure by dietary potassium is attenuated by potassium chloride compared with that of potassium citrate.[6]"
-
Lots of things can cause high blood pressure:
- Adrenaline excess
- Serotonin excess
- NO deficiency
- stimulant abuse
- calcium deficiency
- potassium deficiency
- magnesium deficiency
- RAAS system dysfunction
- estrogen toxicity
- androgen deficiency
- progesterone deficiency
Some of these can have paradoxical effects that result in low or high blood pressure as well, usually through interplay with other systems. A few examples, estrogen toxicity will cause high blood pressure. But a estrogen deficiency will lower nNOS and lead to a higher blood pressure as well. Another example is NO is anti-hypertensive, but too much will result in hypotension. Low blood pressure is more dangerous than a slightly elevated one. Magnesium, by slowing the heart rate, could also cause low BP if taken in high enough dosages. Androgens, especially DHEA, are generally anti-hypertensive by acting through K channels (and to a lesser extent Ca channels). But taking too high of a dose or not supportive by proper nutrition and a enhanced androgenic state could cause too much adrengenic activity, which will increase BP due to excessive adrenaline. This is not an exhaustive list by any means, but just to give you an idea on causes, paradoxes, and just general complexity of something like BP.
-
If changes in blood pressure is sudden suspect iatrogenic causes. Anything that causes vascular damage will do the trick – though sometimes the reaction is delayed. Some examples
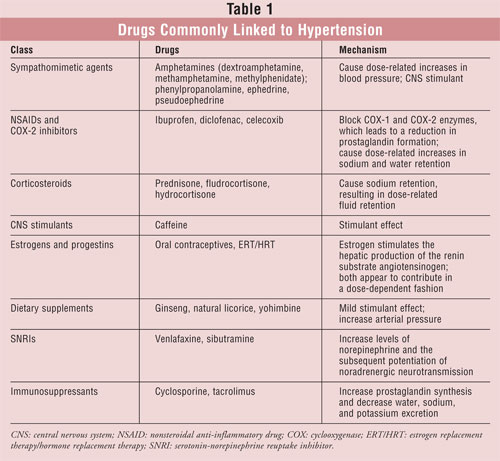
Drug-induced Hypertension: An Unappreciated Cause of Secondary Hypertension
Systemic Inflammatory Response Syndrome Secondary to Nitrofurantoin (hypotension)
Radiation-Association Hypertension in Patients Undergoing Treatment for Prostate Cancer.
Radiation‐Induced Cardiovascular Disease: Review of an Underrecognized Pathology
"Vaccines"
Stage III Hypertension in Patients After mRNA-Based SARS-CoV-2 Vaccination
Blood pressure increase after Pfizer/BioNTech SARS-CoV-2 vaccine
Blood Pressure Increase following COVID-19 Vaccination: A Systematic Overview and Meta-Analysis
-
Awesome guys
thank you. I'll now be reading all this. I already read the first link of the Peat article and I think the PTH angle is especially relevant for the particular person who is complaining of high BP
-
@ursidae
high bp = taurine
Low bp = sodium -
@ursidae Yes, it's a good article. @Peatly linked to the thread where we discussed calcium and it's relation to PTH and high BP. If you're dealing with BP issues that doctors have generally just described as "idiopathic" and therefore trying to prescribe you meds, it may be worth giving calcium a shot first.
Calcium is the most neglected mineral in people's diets now days and according to evidence seems to be the most essential to regulating BP. It was even shown to lower blood pressure in people who were normotensive. Which is pretty profound for a standard little mineral.
I got family history of heart disease, high blood pressure, and kidney disease. I never leave home without my eggshells, lol.
-
Thiamine
Just another consideration.
In this article Lonsdale says this is a hypothesis but it seems like a reasonable one. Pseudo Hypoxia can also be induced by injury or toxins.
Diet Induced Pseudo-Hypoxia and Hypertension
Another thiamine related article
-
@Peatly Thiamine is worth a shot. I've never considered it for a BP intervention before but I do see the logic behind how that would work. Raising glucose oxidation and carbon dioxide will cause vasodilation. That RCT is interesting because the dose is so low. 100mg 3x daily is not that much at all. Which is good because the one concern I've always had with B1 supplementation is the high dosages depleting potassium levels, which would be bad for BP. 300mgs daily would not do this.
-
@Mulloch94 You are correct, high dose thiamine does deplete potassium, or at least increase the requirement. We are not short on potassium on a peaty diet so I don’t worry about it too much. Supplementing thiamine requires balancing with lots of other nutrients.
There are so many things that block oxidative metabolism. I think we can presume that someone with hypertension does have a thiamine deficiency. Even if thiamine deficiency is not the direct cause of hypertension it should help along with other nutrients, for instance magnesium, which works in tandem with thiamine. Magnesium is a calcium channel blocker which lowers PTH unlike most pharmaceutical calcium channel blockers which raises PTH.
Also pufa blocks or depletes thiamine. I learnt about this for the first time from mostlylurking. Frankly, I think injecting pufa into our diets is probably the greatest crime against humanity. Yes, I do believe there is a eugenics depopulation agenda at play. Sorry wrong thread.
-
A Broda Barnes' quote on the role of thyroid in hypertension
Hypertension (high blood pressure) is closely related to kidney function. Goldblatt 30 produced fatal hypertension in dogs many years ago by placing on the kidney artery a simple metal clamp that could be tightened periodically to restrict the flow of blood through the kidney. In hypothyroidism there is a reduction in blood-flow through all the organs including the kidneys. Atherosclerosis in the kidney artery could further reduce the blood flow as effectively as Goldblatt's clamp. Hypertension is very common in hypothyroidism. Rarnes3l has recently reported that thyroid therapy alone was found to relieve 80 percent of the elevated blood pressures seen in a general practice during the past 25 years. Children from patients with hypertension have been found low in thyroid function, and thyroid therapy in the offspring with hypertension has been quite efficacious.
The observations of Andersen leave little doubt that thyroid deficiency can be a potent factor in the genesis of atherosclerosis and hypertension in children. Obviously, if prevention is to be achieved, one must look continually for hypothyroid symptoms from the time of birth. The earlier a diagnosis of hypothyroidism can be made and appropriate therapy started, the better will be the chances of avoiding a premature death from a heart attack. Solved the Riddle of Heart Attacks by Broda Otto Barnes, 1976. Pg. 24-25
-
@Peatly Another interesting correlation that thiamine, magnesium, and calcium all have in common is they increase pyruvate production via upregulating the rate-limited enzyme pyruvate dehydrogenase (PDH). Further suggesting a connection between optimal glucose metabolism and BP control.
In regards to your thyroid statement, Broda Barnes' research is invaluable, and is something pretty everyone should read. Especially if they plan on using thyroid.
But there is other 3rd party data that supports Broda Barnes views, just in case people wanted a second opinion. https://www.nature.com/articles/hr201191#Sec15
"Clinical hypothyroidism is known to increase blood pressure levels, and the main underlying cause of this is thought to be the degree of systemic vascular resistance present in patients with clinical hypothyroidism. T3 can directly act on arterial smooth muscle cells of blood vessels to cause vasodilation. In hypothyroidism, declining T3 levels result in an increased vascular resistance, causing an increase in blood pressure. Hypothyroidism can also lead to abnormal sodium metabolism, increased sympathetic nervous system activity and a decreased glomerular filtration rate, which may contribute to the development of hypertension."
-
@Mulloch94 Excellent
I was looking through my notes and came across this quote about the role of estrogen in blood pressure issues. It’s from an interview called Estrogen vs Progesterone.
The Role Of Estrogen in Blood Pressure Issues
Extract from interview
00:48:33.880 “And the more acute effects of estrogen dominance in the brain can include chorea, sort of uncontrolled, unexpected movements of the arms and legs and such, and epilepsy or seizures are promoted by estrogen. Water retention is really the first action of estrogen on the cell. In exciting it causes it to take up water. Anything that if you block the oxygen delivery to a cell, it'll take up water, too. So the excitation moves the cell's requirements to a level that can't be sustained so the oxygen becomes deficient. It takes up water and shifts its pH and electrical charge. And that same shift of water into the cell makes the walls of the blood vessels leaky to water. And so the water shifts, letting sodium and water both go into the tissues, causing the feet to swell up while you're standing up or during the night your face will share the water burden. The estrogen, that immediate water logging effect, can be compensated by the adrenal, the cortex, and the renin-angiotensin-aldosterone effect, which is to try to compensate for that leakiness by increasing the sodium retention in the kidney. At first, sodium falls in the estrogen dominance as it goes out of the bloodstream into the tissue, but then activating this blood pressure regulating system, you can shift from low blood pressure and swollen feet to high blood pressure and all of the stress-related cortisol-dominant syndrome. Even at an extreme, you can get gangrene constriction of the blood vessels of the extremities and the calcification of soft tissues that the old endocrine textbooks used to mention. That was another thing that Hans Selye investigated in great depth. He called it calciflaxis and calcirgy, in which the excited blood vessels first constrict and load up on calcium. Estrogen releasing histamine and serotonin precedes that, but calcification and then these injured areas tend to load up with iron in most cases, and the iron increases the breakdown-free radical production in these tissues. So, it can lead to such things as gangrene of the fingers and toes and scleroderma, hardening of the skin in various areas that are stressed. I've seen people recover in just a couple of weeks from scleroderma when they stopped using an estrogen supplement............
And progesterone and thyroid are the things that give you the basic long-term protection.” Ray Peat
Question @Mulloch94 - Dr Peat says "at first sodium falls." As the condition progresses does adding extra salt become helpful or harmful?
I'm going to listen to the full interview again
-
@Peatly said in Everything about high blood pressure:
Question @Mulloch94 - Dr Peat says "at first sodium falls." As the condition progresses does adding extra salt become helpful or harmful?
Sounds kind of complicated but it appears he's referring to the water logging effect of estrogen, and how the RAAS steps in to compensate for estrogen's sodium lowering effect.
So if estrogen is activating aldosterone by flushing sodium, and aldosterone tells the kidney's to hold onto sodium, then in my (laymen) opinion is sounds like increasing salt intake solves both of these issues.
The extra salt can both attenuate aldosterone secretion and compensate for estrogen's flushing effects.
However, you should also probably increase potassium as well, because aldosterone's function for holding onto sodium is to dump potassium. So if someone is in this state, it's very likely they're low on potassium, possibly sodium as well, but also they got a unfavorable sodium:potassium balance.
But the underlying cause to all of this is the estrogen dominance to begin with. So that should ultimately be addressed to kill this nasty cycle.
-
@Mulloch94 Thank you. I've noticed increase fluid retention which I think might be related to the potassium/sodium ratio. Frankly, I'm never comfortable throwing salt at problems - I can't manage more than one teaspoon a day. Will increase potassium and see what happens.
-
@Peatly Yeah I don't really enjoy higher salt diets either. Not sure how people do it, too much salt makes my food uneatable. Only things that I can eat with a fair bit of salt are meat and potatoes. Everything else requires just a pinch for me.
It sounds like if I'm reading Ray's views correctly though, salt restricted diets are less dangerous when estrogen isn't high. Taking a few drops of Progest-E may compensate for a lower salt intake by preventing estrogen's flushing mechanism.
I'm not sure what constitutes as "salt restricted," but considering I average around 2,000-2,500mg a day, and the average American is around 4,000mg (or higher for some), I would say my diet is salt restricted.
I don't think eating "DASH" levels of sodium is good per se, they go crazy with it, recommending people eat up to or less than 1,500mgs daily. I think food would be really bland doing that.
And besides, we've already determined extreme salt restriction has - at best - a modest effect on blood pressure. And that eating sufficient amounts of calcium is more likely to bring BP down to manageable levels.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login