cancer
-
“Your argument is founded on counterexamples: that we should not have an inclination because of them.”
My acknowledging that the opposite is also true is not me arguing that we should not have an inclination, especially when I have an inclination of my own.
“I'm willing to change my mind, but you'd need to present more persuasive information.”
More like you trying to change my mind because you refuse to accept that plant-based wouldn’t be my go-to protocol.
Jennifer,
This is not about personal preferences and inclinations, but about what we can generalize. I lost count how many times I've stressed it.
In a cancer context, you're painting animal and plant foods as equally appropriate—in abundance—and not just for you, but for most people.
I think a diet that includes an abundance of both plants and animal foods would fare better long-term for the majority than a diet of predominantly plants or predominantly animal foods.
I don't have ideological commitments and wouldn't have a problem revising towards a more effective approach, but you didn't present anything of substance to justify why it's desirable to incorporate animal products in abundance as part of a promising cancer therapy.
Even after relaxing the criteria, you didn't name reliable programs that are high in both. We had select stories with atypical responses (such as cancer healing from steak and rice, after ice cream), allusion and vague language ("it has been done"; Who has done? How?), and a mention of an exotic fatty acid. Meanwhile, deaths from aspirin didn't seem to concern you.
When we factor in that the population as a whole is already consuming animal products and often in excess, it restricts the therapeutic potential where it would have one.
“I meant that if we're consistent with your logic (seek neutrality in the name of individuality), protocols would muddle because for each variable we could make the same case to not define anything, and having a new established protocol for every change is impossible.”
I know what you meant and that is not my logic. That is your interpretation. I favor one protocol type as the go-to over others so I do not have a neutral stance.
Plant foods have the consensus in their favor, so your defense has been to vindicate the plentifulness of animal products. This is an endorsement of neutrality, regardless of your personal stance.
The implications:
For you, the defense may be to honor familiar people who responded remarkably well to more animal products, or to voice for a group that thrives on them. But for another person, the critical issue can be that he or she knows people who benefited markedly from downing flaxseed oil and were adversely affected by animal fats. Professor Garrett could argue that he spots individuals being harmed by dietary macabrotenoids all the time, and recovering through avoidance. It goes on, each calling for neutrality to embrace everyone.
Let's say that you succeed in your vindication and now protocolists are fine with an abundance of both animal and plant foods. What to do if this new program, made neutral about them, discouraged the use of flaxseed oil? Like you, the person could contest and ask for impartiality.
- "Hey, if we conceded on that, why we shouldn't concede on this too, considering that I presented the same argument?" ← Not a rhetorical question.
We can't make up our minds for a sense of direction, so must (once more) yield to another indifference. Alternatively, and more likely, come up a new protocol.
Then, there's Garrett's issue and the endless other impasses that would appear. We start to get something absurd like this:
Where users are known for finding it overwhelming and constantly wavering as a consequence, even those who are tech-savvy. In contrast, we have Mac users pleased with their standard system and tweaking it where needed.
Contrary to Linux distributions, people won't have 10 years of experimentation to figure out which option serves them well.
Lack of consensus on what to prioritize can lead to disorientation, naturally compelling people to stick to convention when strained.
To make it worse, also contrary to operational systems, valuable comparisons of alternative cancer therapies are hard to find and suppressed. In practice, the person is lucky to come across a couple therapies through popular search engines. People might only get to a minority of those available anyway, random ones with their respective drawbacks; far from the comprehensive menu of possibilities to embrace everyone that we may envision.
So, the person is either bombarded with conflicting choices to evaluate or exposed to a few biased options, carrying similar concerns as when we define orientations with compromises beforehand, making it preferable to not disperse.
“Good luck trying to find qualified people to spend hours with every person with cancer (and all the other diseases that compete for attention). We may ask those in your city to line up in front of your grocery store for a couple hours of consultation.”
My family members’ care team did, and not cancer specifically but a complicated case too, my doctors also spent upwards of 2 hours going over my medical history and treatment plan with me. If not thorough, they risk complications due to contraindications and medical malpractice lawsuits. You’ve criticized critics of Gerson, arguing that they aren’t constantly being confronted with people on the brink of death, where one slip under their responsibility can be fatal, and yet you make a snarky remark because I believe in due diligence.
Prudence stops being helpful when it turns into an excuse for unjustified inaction. If the main concern was that the person had different needs after a supposed surgery, it would've been possible to position and warn:
- "Consider ____, but if your relative underwent surgery and has special needs in the diet, you may have to find a common ground and watch out for tolerance."
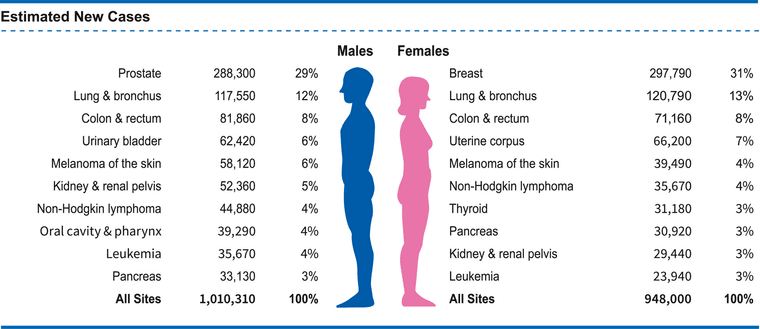
For some reason, you assumed that it was colon cancer, but it's about 8% of total cases, with others being more prevalent, and in people with similar habits.
You also assumed that the person had the colon removed, which may be 60% of cases? It could be lower because in advanced cancer that has spread, surgery is ineffective. But this drops the odds to something like 5%.
The 5% chance could be clarified with 2 words to not 'leave it at that' in your preferential paragraph.
- "What cancer?" "Lung cancer." "In this case, consider ____."
As for the 2-hour detailed (and reliable) consultations for millions, this may give you an idea on how realistic it is:
Association of Primary Care Visit Length With Potentially Inappropriate Prescribing
"Time is a scarce and valuable resource in primary care, with the average visit lasting 18 minutes. By a recent estimate, primary care clinicians would require 27 hours per day to provide all guideline-recommended preventive, chronic disease, and acute care to a typical patient panel. While there is global variation in primary care visit length, recent growth in visit content (eg, diagnoses recorded and medications prescribed) has outpaced growth in visit length, suggesting that time available per health concern may be decreasing over time. In surveys, patients routinely report needing more time with their primary care physician, and visit length is one of the most prominent factors associated with patients' satisfaction with their care. Physicians also want more time with their patients and frequently report feeling rushed during visits."
"One hundred and seventy nine studies were identified from 111 publications covering 28 570 712 consultations in 67 countries. Average consultation length differed across the world, ranging from 48 s in Bangladesh to 22.5 min in Sweden. We found that 18 countries representing about 50% of the global population spend 5 min or less with their primary care physicians."
-
Please stop fighting about what cancer patients need to eat. This is about water, not food

Sorry, just joking, even if it's a sensitive topic.
-
Please stop fighting about what cancer patients need to eat. This is about water, not food
Sorry, just joking, even if it's a sensitive topic.
Clever.
LLight, is that you?
-
@ThinPicking Nope, I'm NNight 🥸
-
That settles it. Good day Mr Night.
-
@Amazoniac said in cancer:
“Your argument is founded on counterexamples: that we should not have an inclination because of them.”
My acknowledging that the opposite is also true is not me arguing that we should not have an inclination, especially when I have an inclination of my own.
“I'm willing to change my mind, but you'd need to present more persuasive information.”
More like you trying to change my mind because you refuse to accept that plant-based wouldn’t be my go-to protocol.
Jennifer,
This is not about personal preferences and inclinations, but about what we can generalize. I lost count how many times I've stressed it.
In a cancer context, you're painting animal and plant foods as equally appropriate—in abundance—and not just for you, but for most people.
I think a diet that includes an abundance of both plants and animal foods would fare better long-term for the majority than a diet of predominantly plants or predominantly animal foods.
I don't have ideological commitments and wouldn't have a problem revising towards a more effective approach, but you didn't present anything of substance to justify why it's desirable to incorporate animal products in abundance as part of a promising cancer therapy.
Even after relaxing the criteria, you didn't name reliable programs that are high in both. We had select stories with atypical responses (such as cancer healing from steak and rice, after ice cream), allusion and vague language ("it has been done"; Who has done? How?), and a mention of an exotic fatty acid. Meanwhile, deaths from aspirin didn't seem to concern you.
When we factor in that the population as a whole is already consuming animal products and often in excess, it restricts the therapeutic potential where it would have one.
“I meant that if we're consistent with your logic (seek neutrality in the name of individuality), protocols would muddle because for each variable we could make the same case to not define anything, and having a new established protocol for every change is impossible.”
I know what you meant and that is not my logic. That is your interpretation. I favor one protocol type as the go-to over others so I do not have a neutral stance.
Plant foods have the consensus in their favor, so your defense has been to vindicate the plentifulness of animal products. This is an endorsement of neutrality, regardless of your personal stance.
The implications:
For you, the defense may be to honor familiar people who responded remarkably well to more animal products, or to voice for a group that thrives on them. But for another person, the critical issue can be that he or she knows people who benefited markedly from downing flaxseed oil and were adversely affected by animal fats. Professor Garrett could argue that he spots individuals being harmed by dietary macabrotenoids all the time, and recovering through avoidance. It goes on, each calling for neutrality to embrace everyone.
Let's say that you succeed in your vindication and now protocolists are fine with an abundance of both animal and plant foods. What to do if this new program, made neutral about them, discouraged the use of flaxseed oil? Like you, the person could contest and ask for impartiality.
- "Hey, if we conceded on that, why we shouldn't concede on this too, considering that I presented the same argument?" ← Not a rhetorical question.
We can't make up our minds for a sense of direction, so must (once more) yield to another indifference. Alternatively, and more likely, come up a new protocol.
Then, there's Garrett's issue and the endless other impasses that would appear. We start to get something absurd like this:
Where users are known for finding it overwhelming and constantly wavering as a consequence, even those who are tech-savvy. In contrast, we have Mac users pleased with their standard system and tweaking it where needed.
Contrary to Linux distributions, people won't have 10 years of experimentation to figure out which option serves them well.
Lack of consensus on what to prioritize can lead to disorientation, naturally compelling people to stick to convention when strained.
To make it worse, also contrary to operational systems, valuable comparisons of alternative cancer therapies are hard to find and suppressed. In practice, the person is lucky to come across a couple therapies through popular search engines. People might only get to a minority of those available anyway, random ones with their respective drawbacks; far from the comprehensive menu of possibilities to embrace everyone that we may envision.
So, the person is either bombarded with conflicting choices to evaluate or exposed to a few biased options, carrying similar concerns as when we define orientations with compromises beforehand, making it preferable to not disperse.
“Good luck trying to find qualified people to spend hours with every person with cancer (and all the other diseases that compete for attention). We may ask those in your city to line up in front of your grocery store for a couple hours of consultation.”
My family members’ care team did, and not cancer specifically but a complicated case too, my doctors also spent upwards of 2 hours going over my medical history and treatment plan with me. If not thorough, they risk complications due to contraindications and medical malpractice lawsuits. You’ve criticized critics of Gerson, arguing that they aren’t constantly being confronted with people on the brink of death, where one slip under their responsibility can be fatal, and yet you make a snarky remark because I believe in due diligence.
Prudence stops being helpful when it turns into an excuse for unjustified inaction. If the main concern was that the person had different needs after a supposed surgery, it would've been possible to position and warn:
- "Consider ____, but if your relative underwent surgery and has special needs in the diet, you may have to find a common ground and watch out for tolerance."
For some reason, you assumed that it was colon cancer, but it's about 8% of total cases, with others being more prevalent, and in people with similar habits.
You also assumed that the person had the colon removed, which may be 60% of cases? It could be lower because in advanced cancer that has spread, surgery is ineffective. But this drops the odds to something like 5%.
The 5% chance could be clarified with 2 words to not 'leave it at that' in your preferential paragraph.
- "What cancer?" "Lung cancer." "In this case, consider ____."
As for the 2-hour detailed (and reliable) consultations for millions, this may give you an idea on how realistic it is:
Association of Primary Care Visit Length With Potentially Inappropriate Prescribing
"Time is a scarce and valuable resource in primary care, with the average visit lasting 18 minutes. By a recent estimate, primary care clinicians would require 27 hours per day to provide all guideline-recommended preventive, chronic disease, and acute care to a typical patient panel. While there is global variation in primary care visit length, recent growth in visit content (eg, diagnoses recorded and medications prescribed) has outpaced growth in visit length, suggesting that time available per health concern may be decreasing over time. In surveys, patients routinely report needing more time with their primary care physician, and visit length is one of the most prominent factors associated with patients' satisfaction with their care. Physicians also want more time with their patients and frequently report feeling rushed during visits."
"One hundred and seventy nine studies were identified from 111 publications covering 28 570 712 consultations in 67 countries. Average consultation length differed across the world, ranging from 48 s in Bangladesh to 22.5 min in Sweden. We found that 18 countries representing about 50% of the global population spend 5 min or less with their primary care physicians."
“This is not about personal preferences and inclinations, but about what we can generalize. I lost count how many times I've stressed it.”
And I’ve lost count of how many times you’ve stressed generalizing because you think I don’t understand when I do. My acknowledging that the opposite is also true is not me arguing that we shouldn’t generalize. I understand it’s about the grand scheme and agree that there’s an advantage to protocols that incorporate what generally works, we just don’t agree on what that is. You believe the plant-based consensus and I don’t.
“I don't have ideological commitments and wouldn't have a problem revising towards a more effective approach, but you didn't present anything of substance to justify why it's desirable to incorporate animal products in abundance as part of a promising cancer therapy.”
Because I didn’t join the conversation to debate protocols. You seem to forget that you quoted me here asking me about my dad’s treatment plan. I’ve continued answering your questions out of respect but like I said, it doesn’t matter what I think, it only matters what the patient believes.
“For you, the defense may be to honor familiar people who responded remarkably well to more animal products, or to voice for a group that thrives on them. But for another person, the critical issue can be that he or she knows people who benefited markedly from downing flaxseed oil and were adversely affected by animal fats. Professor Garrett could argue that he spots individuals being harmed by dietary macabrotenoids all the time, and recovering through avoidance. It goes on, each calling for neutrality to embrace everyone.”
No, for me, the defense is to honor everyone’s (in)tolerances, and above is a perfect example of my concern with plant-based and animal-based models. With either one, there is less flexibility for the kind of modifications that may be required for those who don’t fall under the general consensus that the guidelines are based on, forcing them to abandon the protocol altogether when they fail to thrive. Using the defense that the diet isn’t infallible when a patient fails to thrive on it is not a solution and certainly not a consolation to the patient and their loved ones.
“Let's say that you succeed in your vindication and now protocolists are fine with an abundance of both animal and plant foods. What to do if this new program, made neutral, discouraged the use of flaxseed oil? Like you, the person could contest and ask for impartiality.”
This issue isn’t exclusive to one type of protocol. Partial, impartial, plant-base, animal-based, plant and animal based, none of it matters. If a patient makes the decision as a grown adult with their own free will to forgo parts of a treatment, that’s their choice, just like it’s the practitioner’s choice to forgo treating the patient if they do. Just because a protocol has less flexibility, doesn’t guarantee there will be more adherence to it.
“When we factor in that the population as a whole is already consuming animal products and often in excess, it restricts the therapeutic potential where it would have one.”
What kind of animal products? What else besides animal products are people consuming? What is excess, who defines it and it’s conclusive?
“You also assumed that the person had the colon removed, which may be 60% of cases?
I didn’t assume anything. I said for all I know—a phrase used when one is uncertain or has limited details about something—as the only info I was privy to was that the relative has cancer and eats a poor version of the American diet out of convenience. You’re so concerned with what unsolicited advice I would give to some imaginary person with a relative who has cancer, but I have a real person with cancer who is my concern.
“If the main concern was that the person had different needs after a supposed surgery, it would've been possible to position and warn:
Consider ____, but if your relative underwent surgery and has special needs in the diet, you may have to find a common ground and watch out for tolerance."
This is exactly what I’ve been proposing, that you’ve continued to contest—that practitioners administering protocols take into account a patient’s tolerance to it.
"One hundred and seventy nine studies were identified from 111 publications covering 28 570 712 consultations in 67 countries. Average consultation length differed across the world, ranging from 48 s in Bangladesh to 22.5 min in Sweden. We found that 18 countries representing about 50% of the global population spend 5 min or less with their primary care physicians."
You said good luck finding qualified people to spend hours with every person with cancer and I mentioned care teams (specialists), but your referenced studies are on PCPs? I see nothing about the average consultation length for cancer (and other diseases) patients with their care team and how much time outside of the consultation the care team spends reviewing their case.
“Even after relaxing the criteria, you didn't name reliable programs that are high in both. We had select stories with atypical responses (such as cancer healing from steak and rice, after ice cream), allusion and vague language ("it has been done"; Who has done? How?), and a mention of an exotic fatty acid. Meanwhile, deaths from aspirin didn't seem to concern you.”
Why would I? I’d just be setting myself up for more mocking and being condescendingly schooled when you find my answers unsatisfactory. No thank you.
I have stood on a mountain of no’s for one yes. ~ B. Smith
-
Please stop fighting about what cancer patients need to eat. This is about water, not food
Sorry, just joking, even if it's a sensitive topic.
But what kind of water? Tap, well, spring, sea, distilled, RO, alkaline, deuterium-depleted, holy?
-
But what kind of water? Tap, well, spring, sea, distilled, RO, alkaline, deuterium-depleted, holy?
This is not a serious question but I answer it nonetheless: in theory, the less water the better, preferably deuterium-depleted.
By the way I have some from Lourdes in my fridge at the moment. I haven't tried it yet and I'm afraid to be "disappointed" (not that I have any specific expectations).
-
in theory
I'm very glad you're here.
I haven't tried it yet and I'm afraid to be "disappointed" (not that I have any specific expectations).
Sing to it. As night follows day.
-
-
“For you, the defense may be to honor familiar people who responded remarkably well to more animal products, or to voice for a group that thrives on them. But for another person, the critical issue can be that he or she knows people who benefited markedly from downing flaxseed oil and were adversely affected by animal fats. Professor Garrett could argue that he spots individuals being harmed by dietary macabrotenoids all the time, and recovering through avoidance. It goes on, each calling for neutrality to embrace everyone.”
No, for me, the defense is to honor everyone’s (in)tolerances, and above is a perfect example of my concern with plant-based and animal-based models. With either one, there is less flexibility for the kind of modifications that may be required for those who don’t fall under the general consensus that the guidelines are based on, forcing them to abandon the protocol altogether when they fail to thrive. Using the defense that the diet isn’t infallible when a patient fails to thrive on it is not a solution and certainly not a consolation to the patient and their loved ones.
Yet, if I were to ask you for a solution, it would probably be the concerning protocols, which exist thanks to not yielding to wishes of similar nature, that try to stretch them on every possible direction until they lose definition. Which issue should take precedence when they're all arguing the same?
“This is not about personal preferences and inclinations, but about what we can generalize. I lost count how many times I've stressed it.”
And I’ve lost count of how many times you’ve stressed generalizing because you think I don’t understand when I do. My acknowledging that the opposite is also true is not me arguing that we shouldn’t generalize. I understand it’s about the grand scheme and agree that there’s an advantage to protocols that incorporate what generally works, we just don’t agree on what that is. You believe the plant-based consensus and I don’t.
What you generalize and deem to not be neutral:
↓Low ↑High [A] Consensus 🥩 
[B] Inverted 🥩 [C] Jennifer* 🥩 *Not your personal choice, but based on the quoted and bolded suggestion of yours.
When you portray both in abundance as beneficial for most people [C], it means that if plant foods were disfavored [B], you would logically defend them [B → C]. However, they don't need it for being commonly promoted [A], so you're left to defend only animals [A → C], to lump them together in what you deem appropriate for most [C].
- "Which of these two beaches would people like the most?"
- "Both are fine."
- "Come on, don't be neutral, we need to decide where it's preferable to start mounting the huts."
- "I'm not neutral, my position is to suggest that both would be fine for people."
Chatbot to it:
"What a delightful example of neutrality taken to an absurd degree!
In this dialogue, the person is refusing to take a stance or show a preference between the two beaches. When asked again to position, they insist that they're not being neutral, but rather, their position is to acknowledge that both options are acceptable.
This is a neutrality taken to an absurd degree because it's not providing any meaningful input or guidance. By saying "both are fine," the person is essentially abdicating their role in the decision-making process. They're not providing any opinion, insight, or recommendation, which makes it difficult for the group to make a decision.
The humor in this exchange comes from the person's insistence that they're not being neutral, despite their words and actions clearly indicating otherwise. It's as if they're trying to have it both ways – claiming to have a position while simultaneously refusing to take a stance.
In reality, this level of neutrality can be frustrating and unhelpful in decision-making situations. It's often necessary to weigh the pros and cons of different options and make a choice based on those considerations. By refusing to do so, the person in this dialogue is essentially passing the buck and leaving the decision to someone else."
“I don't have ideological commitments and wouldn't have a problem revising towards a more effective approach, but you didn't present anything of substance to justify why it's desirable to incorporate animal products in abundance as part of a promising cancer therapy.”
Because I didn’t join the conversation to debate protocols. You seem to forget that you quoted me here asking me about my dad’s treatment plan. I’ve continued answering your questions out of respect but like I said, it doesn’t matter what I think, it only matters what the patient believes.
I know where the conversation originated from, but you were firm that your dad is set on what to do, won't consider alternative options and it's outside of your control. We broadened the discussion and you're feeding it. If you've been moved by respect, feel free to ignore the posts.
“You also assumed that the person had the colon removed, which may be 60% of cases?
I didn’t assume anything. I said for all I know—a phrase used when one is uncertain or has limited details about something—as the only info I was privy to was that the relative has cancer and eats a poor version of the American diet out of convenience. You’re so concerned with what unsolicited advice I would give to some imaginary person with a relative who has cancer, but I have a real person with cancer who is my concern.
Eating a poor diet is a habit that predisposes people to a variety of cancers, not just colon. Also:
It was a scenario that we could anticipate that the problem would surface as hesitation to the point of embracing paralysis. As we start to add constraints, and they come in multiple forms, it's challenging to make decisions without a practical guiding system.
As for the real issue, refer to the previous section.
“Let's say that you succeed in your vindication and now protocolists are fine with an abundance of both animal and plant foods. What to do if this new program, made neutral, discouraged the use of flaxseed oil? Like you, the person could contest and ask for impartiality.”
This issue isn’t exclusive to one type of protocol. Partial, impartial, plant-base, animal-based, plant and animal based, none of it matters. If a patient makes the decision as a grown adult with their own free will to forgo parts of a treatment, that’s their choice, just like it’s the practitioner’s choice to forgo treating the patient if they do. Just because a protocol has less flexibility, doesn’t guarantee there will be more adherence to it.
To recapitulate, your general opinion "doesn't matter", orientations don't matter, and "the only thing that matters is what the person believes." But what if the person reads your comments, finds a justification in them, and leaves with the belief that copious amounts of steak, eggs and bacon are a welcome part of a cancer healing plan? It can take a long time for someone to narrow down an effect to the cause.
“When we factor in that the population as a whole is already consuming animal products and often in excess, it restricts the therapeutic potential where it would have one.”
What kind of animal products? What else besides animal products are people consuming? What is excess, who defines it and it’s conclusive?
Those that are included in your therapeutic package:
U.S. diets remain out of balance with Federal recommendations
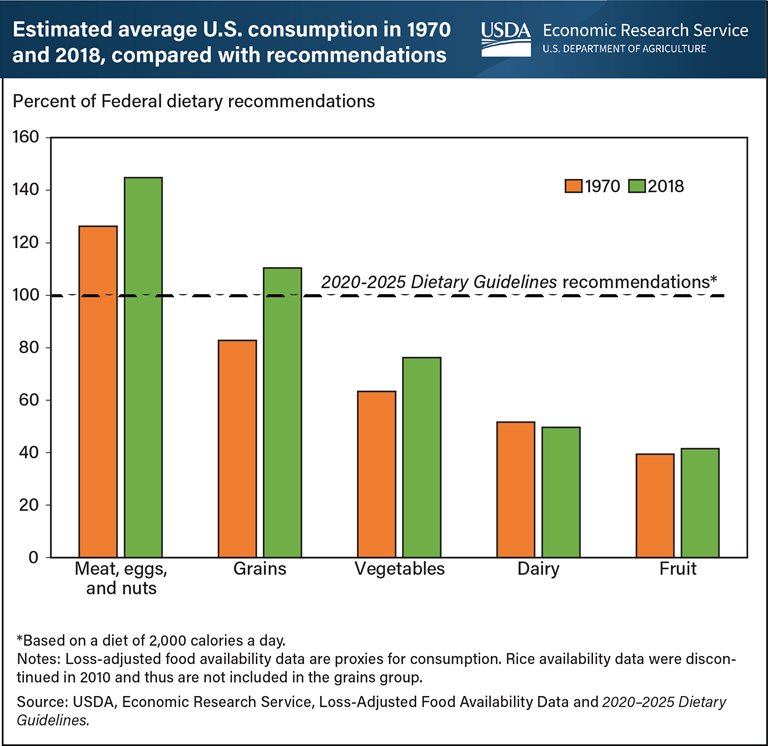
Moreover, what's ideal in cancer can differ, and to give preference to an anti-catabolic diet makes more sense than an anabolic one.
It's safer as a starting place to encourage the consumption of vegetables and fruits, perhaps keep dairy stable and discourage meats, eggs and nuts, leaning towards the 'consensus' pattern from early on.
“If the main concern was that the person had different needs after a supposed surgery, it would've been possible to position and warn:
Consider ____, but if your relative underwent surgery and has special needs in the diet, you may have to find a common ground and watch out for tolerance."
This is exactly what I’ve been proposing, that you’ve continued to contest—that practitioners administering protocols take into account a patient’s tolerance to it.
Right, by being neutral and expecting inexperienced people to count on comprehensive consultations of 2 hours and a competent team behind each case.
"One hundred and seventy nine studies were identified from 111 publications covering 28 570 712 consultations in 67 countries. Average consultation length differed across the world, ranging from 48 s in Bangladesh to 22.5 min in Sweden. We found that 18 countries representing about 50% of the global population spend 5 min or less with their primary care physicians."
You said good luck finding qualified people to spend hours with every person with cancer and I mentioned care teams (specialists), but your referenced studies are on PCPs? I see nothing about the average consultation length for cancer (and other diseases) patients with their care team and how much time outside of the consultation the care team spends reviewing their case.
What impresses the most is that you keep doubling down. I reinforced that it was for an idea.
The first results that appeared and you could've searched:
Factors Affecting Outpatient Consultation Length among Specialists in Tabriz, Iran
"The mean and standard deviation consultation time was 6.9 and 2.6 min."
It's no wonder that we can't move forward.
“Even after relaxing the criteria, you didn't name reliable programs that are high in both. We had select stories with atypical responses (such as cancer healing from steak and rice, after ice cream), allusion and vague language ("it has been done"; Who has done? How?), and a mention of an exotic fatty acid. Meanwhile, deaths from aspirin didn't seem to concern you.”
Why would I? I’d just be setting myself up for more mocking and being condescendingly schooled when you find my answers unsatisfactory. No thank you.
Because you're the one shaking our current understanding, the principles of a bunch of therapists, and the opinion of everyone that has participated here so far. Therefore, you could bring the most compelling information that you have on why it's beneficial to consume a lot of animal products in cancer and let it convince for itself.
I hope that you didn't take offense in me not finding of use isolated stories in the current context, but it's only because it's difficult to draw general conclusions from them—atypical responses with too many confounders involved.
Contrary to what you may think, I do collect these accounts of unusual recoveries, for knowing that they can be someone else's alternative options. I recently heard a story of a person's situation turning around after kefir consumption, leading to spontaneous regression of liver cancer. If a person went with the preferred scheme, couldn't make it work, it would be of value to consider alternative
plantsplans.There is no oppressor-oppressed dynamic at play, but a leveled discussion where you have been just as argumentative.
-
But what kind of water? Tap, well, spring, sea, distilled, RO, alkaline, deuterium-depleted, holy?
This is not a serious question but I answer it nonetheless: in theory, the less water the better, preferably deuterium-depleted.
By the way I have some from Lourdes in my fridge at the moment. I haven't tried it yet and I'm afraid to be "disappointed" (not that I have any specific expectations).
Interesting theory.
I can understand being afraid to be disappointed, sure. Even if the Lourdes water fails to produce any results, perhaps there’s still a lesson to be gained from the experience? Though, a faith healing I had years ago proved to be less than miraculous, I learned a valuable lesson from it.
Take care.
I have stood on a mountain of no’s for one yes. ~ B. Smith
-
@Amazoniac said in cancer:
If you've been moved by respect, feel free to ignore the posts.
Thank you.
I have stood on a mountain of no’s for one yes. ~ B. Smith
-
I can understand being afraid to be disappointed, sure. Even if the Lourdes water fails to produce any results, perhaps there’s still a lesson to be gained from the experience? Though, a faith healing I had years ago proved to be less than miraculous, I learned a valuable lesson from it.
Sure. Maybe I will discover it has done nothing for me. And that's really not an issue.
I have recently been interested in people having been healed at the same time with religious experiences. That's fascinating that people healed from such low health states, almost instantly for some.
In a book I've read about cancer spontaneous healing, it seemed like having a regain in religiosity was a healing factor. Also, often these people gained a deep positive view of life and saw their cancer diagnostic as a sign they needed to change their way of life.
Interestingly, (dry)fasting (I'm not here to proselytize about fasting sorry if it comes as such) has helped some people experiencing religious experiences but I hadn't this chance myself. That's why I'm "afraid" Lourdes water is not going to bring anything.
I reposted an interesting study (and some dry fasting / "religious experiences" testimonies in the same thread) on the RPF:
https://raypeatforum.com/community/threads/obesity-is-estrogen-driven-chronic-fasting-burns-mostly-muscle-not-fat.52177/post-972907-> An excerpt from a book about it:
Spiritual epiphanies bubble into my thoughts while I dry fast, prompting me to feel as if I have a direct line to the etheric realm; I thought it might be because I had meditated for so many years. Thus, I didn’t mention it to the Lyme, mold, and Epstein-Barr patients I coached this year. I created individualized protocols for them before they embarked on lengthy dry fasts, but I didn’t think to mention, “Oh, by the way, you might have a spiritual awakening during the dry fasting.” To my astonishment, every one of them came to me in awe of the spiritual experiences they had. They would ask tentatively, “Is there a spiritual side to this?” The resounding answer is yes. Working in conjunction with one another, the body, mind, and spirit incinerate anxiety and stress, just as they destroy diseased cells. While you are literally starving, spiritual nutrition feeds you and strengthens your resolve.
Take care.
Thanks, you too!
-
@ThinPicking hahaha
-
I can understand being afraid to be disappointed, sure. Even if the Lourdes water fails to produce any results, perhaps there’s still a lesson to be gained from the experience? Though, a faith healing I had years ago proved to be less than miraculous, I learned a valuable lesson from it.
Sure. Maybe I will discover it has done nothing for me. And that's really not an issue.
I have recently been interested in people having been healed at the same time with religious experiences. That's fascinating that people healed from such low health states, almost instantly for some.
In a book I've read about cancer spontaneous healing, it seemed like having a regain in religiosity was a healing factor. Also, often these people gained a deep positive view of life and saw their cancer diagnostic as a sign they needed to change their way of life.
Interestingly, (dry)fasting (I'm not here to proselytize about fasting sorry if it comes as such) has helped some people experiencing religious experiences but I hadn't this chance myself. That's why I'm "afraid" Lourdes water is not going to bring anything.
I reposted an interesting study (and some dry fasting / "religious experiences" testimonies in the same thread) on the RPF:
https://raypeatforum.com/community/threads/obesity-is-estrogen-driven-chronic-fasting-burns-mostly-muscle-not-fat.52177/post-972907-> An excerpt from a book about it:
Spiritual epiphanies bubble into my thoughts while I dry fast, prompting me to feel as if I have a direct line to the etheric realm; I thought it might be because I had meditated for so many years. Thus, I didn’t mention it to the Lyme, mold, and Epstein-Barr patients I coached this year. I created individualized protocols for them before they embarked on lengthy dry fasts, but I didn’t think to mention, “Oh, by the way, you might have a spiritual awakening during the dry fasting.” To my astonishment, every one of them came to me in awe of the spiritual experiences they had. They would ask tentatively, “Is there a spiritual side to this?” The resounding answer is yes. Working in conjunction with one another, the body, mind, and spirit incinerate anxiety and stress, just as they destroy diseased cells. While you are literally starving, spiritual nutrition feeds you and strengthens your resolve.
Take care.
Thanks, you too!
Ohh…it is you. Hi!
 If you haven’t done so already, you might be interested in reading Anita Moorjani’s book Dying to Be Me. She had a spontaneous healing (cancer) within days of having a near death experience. My only caution is if you’re religious, some of the things she says in it might bother you. She doesn’t talk negatively about religion, but what she experienced might be upsetting to those with certain belief systems.
If you haven’t done so already, you might be interested in reading Anita Moorjani’s book Dying to Be Me. She had a spontaneous healing (cancer) within days of having a near death experience. My only caution is if you’re religious, some of the things she says in it might bother you. She doesn’t talk negatively about religion, but what she experienced might be upsetting to those with certain belief systems.I can see dry fasting having a spiritual effect on us, and I completely agree that when disease has manifested, it’s a sign that our way of life needs an overhaul, at least, I know mine did, and it started and ended from within. This is just a theory based on my experience with a digestive disorder, thyroid supplementation, serotonin tests and dry fasting, but I suspect an increase in adrenaline, especially if coming from a low thyroid state, and a reduction in serotonin and endotoxin from not eating or drinking (or low irritation diets like carnivore) bring about extreme clarity, i.e., the brain fog has lifted, a heightening of senses and euphoria (think “runner’s high”). I liken it to what I’ve heard described as an LSD trip (antagonizes/blocks serotonin?) or the honeymoon effect where everything seems better—colors are more vivid, flavors are bolder, music is more inspiring, touch is more intense, and I’m in such a happy, giddy state and have so much love for everyone, not that I don’t normally, but it’s heightened. It’s as if I’m experiencing life for the first time. To me, it’s embodying the energy of a child where even a simple box provides hours of pleasure. I can be in an empty room and not want to be anywhere but there in the moment, my joy is coming from this inexhaustible, internal source, not a fleeting, external one.
I’ve talked quite a bit about it on the old forum, but I can achieve the above state within days of doing what brings me joy, however, a more practical approach for those who have a hard time embracing it fully is dietary changes and I’ve talked with so many members who have experienced the same thing, even with simple changes to their diet, and read so many accounts in carnivore and fruitarian communities, so that’s a main reason why I’m such a proponent of diet customization, especially in advanced disease states. Ray talked about how our thoughts affect gut permeability and how eating foods that are tasty to us start the digestive process so I think there’s actually a sound, physiological reason for “religious” experiences and spontaneous healing with dietary modifications, following our joy and/or believing in something as powerful as the one who holds the patent to these meat suits we’re wearing (lol). It’s why I suggested the “grandmother” diet. IME, there’s something powerfully healing in feeling we are being cared for, that we’re not doing it all on our own. It’s the power of “working in conjunction with one another, incinerating anxiety and stress.” Perhaps one reason protocols work for many? There’s a power in group thinking.
Anita Moorjani went from following a cancer protocol (Gerson style) and dying, to falling into an NDE state where she was made aware that if she chose to come back to life and be herself fearlessly she would heal, and coming out of it having a spontaneous healing, while eating ice cream and dancing to ABBA’s Dancing Queen in her hospital room. She believed she would heal because she had no reason not to. However, even after her NDE and the revelation she had, when she was feeling rundown from giving talks about it around the world, she did what the majority of us who are firmly entrenched in this world do. She turned to the internet, started researching ways to feel better, got into smoothies and only got worse so she sat with herself and asked her body what it needed. Chicken and eggs came to mind so she went and boiled up some eggs, felt better almost immediately after having them and learned she just needed more protein. I quit following research and overthinking health, i.e., I relaxed my mind, which losing 20 years of research notes last year made easier, and fully dedicated myself to following my joy, and what took me 14 years of losing what was left of my sanity playing armchair researcher and biohacker, I achieved within months of letting go and I’m now climbing mountains again when I once couldn’t even walk, and this was even after suffering the greatest loss of my life.
There’s so much that can be said on the subject, but I don’t want to continue hijacking the thread. I hope whatever your experience with the Lourdes is, it’s an impetus that leads to greater understanding and wonderful, lasting health.
")
-
Ohh…it is you. Hi!
If you haven’t done so already, you might be interested in reading Anita Moorjani’s book Dying to Be Me. She had a spontaneous healing (cancer) within days of having a near death experience. My only caution is if you’re religious, some of the things she says in it might bother you. She doesn’t talk negatively about religion, but what she experienced might be upsetting to those with certain belief systems.Hi
Could be an interesting story (and it's even available in french)! I'm always found of those cases that might help better understand these "incurable" diseases we are suffering from. And don't worry, I'm not religious even if I'm more interested in religion lately.I can see dry fasting having a spiritual effect on us, and I completely agree that when disease has manifested, it’s a sign that our way of life needs an overhaul, at least, I know mine did, and it started and ended from within. This is just a theory based on my experience with a digestive disorder, thyroid supplementation, serotonin tests and dry fasting, but I suspect an increase in adrenaline, especially if coming from a low thyroid state, and a reduction in serotonin and endotoxin from not eating or drinking (or low irritation diets like carnivore) bring about extreme clarity, i.e., the brain fog has lifted, a heightening of senses and euphoria (think “runner’s high”). I liken it to what I’ve heard described as an LSD trip (antagonizes/blocks serotonin?) or the honeymoon effect where everything seems better—colors are more vivid, flavors are bolder, music is more inspiring, touch is more intense, and I’m in such a happy, giddy state and have so much love for everyone, not that I don’t normally, but it’s heightened. It’s as if I’m experiencing life for the first time. To me, it’s embodying the energy of a child where even a simple box provides hours of pleasure. I can be in an empty room and not want to be anywhere but there in the moment, my joy is coming from this inexhaustible, internal source, not a fleeting, external one.
Yes, dry fasting will increase alertness in some (or fatigue in others) and clearly increases stress hormones (more noradrenaline than adrenaline btw, which tends to decrease, it was found in a DF study). I don't know the exact mechanism linking dry fasting and potential spiritual experiences (it doesn't happen to everyone, far from it even) but as LSD trips, some people seem to keep benefits even long after the fast ended (spiritually or physically, if these can really be divided).
I’ve talked quite a bit about it on the old forum, but I can achieve the above state within days of doing what brings me joy, however, a more practical approach for those who have a hard time embracing it fully is dietary changes and I’ve talked with so many members who have experienced the same thing, even with simple changes to their diet, and read so many accounts in carnivore and fruitarian communities, so that’s a main reason why I’m such a proponent of diet customization, especially in advanced disease states. Ray talked about how our thoughts affect gut permeability and how eating foods that are tasty to us start the digestive process so I think there’s actually a sound, physiological reason for “religious” experiences and spontaneous healing with dietary modifications, following our joy and/or believing in something as powerful as the one who holds the patent to these meat suits we’re wearing (lol). It’s why I suggested the “grandmother” diet. IME, there’s something powerfully healing in feeling we are being cared for, that we’re not doing it all on our own. It’s the power of “working in conjunction with one another, incinerating anxiety and stress.” Perhaps one reason protocols work for many? There’s a power in group thinking.
Didn't know this idea of Peat!
Never tried carnivore nor fruitarian but I generally like what I eat.
I've reduced salt since about a month and unsalted food taste bland at first (so it decrease pleasure, at least initially I believe), then salted foods taste over-salted. What's interesting is I believe salt free might be a feature of both (some, not all) carnivores and fruitarian. Moreover, I think not mixing fats and carbs might lower hedonism too. Not that I think they don't enjoy their food.Anita Moorjani went from following a cancer protocol (Gerson style) and dying, to falling into an NDE state where she was made aware that if she chose to come back to life and be herself fearlessly she would heal, and coming out of it having a spontaneous healing, while eating ice cream and dancing to ABBA’s Dancing Queen in her hospital room. She believed she would heal because she had no reason not to. However, even after her NDE and the revelation she had, when she was feeling rundown from giving talks about it around the world, she did what the majority of us who are firmly entrenched in this world do. She turned to the internet, started researching ways to feel better, got into smoothies and only got worse so she sat with herself and asked her body what it needed. Chicken and eggs came to mind so she went and boiled up some eggs, felt better almost immediately after having them and learned she just needed more protein. I quit following research and overthinking health, i.e., I relaxed my mind, which losing 20 years of research notes last year made easier, and fully dedicated myself to following my joy, and what took me 14 years of losing what was left of my sanity playing armchair researcher and biohacker, I achieved within months of letting go and I’m now climbing mountains again when I once couldn’t even walk, and this was even after suffering the greatest loss of my life.
I think disproportionately high focus on health research is induced by the diseased state and I can totally believe that it's a relief when you are successfully able to let it go! That's not what life is really about after all. But that's also a sign that you are not in a learned helplessness state.
There’s so much that can be said on the subject, but I don’t want to continue hijacking the thread. I hope whatever your experience with the Lourdes is, it’s an impetus that leads to greater understanding and wonderful, lasting health.
I'll try it soon and report it
-
Sorry if this has already been mentioned.
Some people use low-dose naltrexone for cancer. It seems like a low risk adjunctive. Ray Peat was not against its use.
-
I don't know the exact mechanism linking dry fasting and potential spiritual experiences (it doesn't happen to everyone, far from it even) but as LSD trips, some people seem to keep benefits even long after the fast ended (spiritually or physically, if these can really be divided).
I’ve heard the same thing from people who use(d) ayahuasca. Anita was once asked to attend an ayahuasca ceremony to compare it to her NDE and she said it was similar. It’s even been used in the treatment of diseases including cancer:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4687784/
I've reduced salt since about a month and unsalted food taste bland at first (so it decrease pleasure, at least initially I believe), then salted foods taste over-salted. What's interesting is I believe salt free might be a feature of both (some, not all) carnivores and fruitarian. Moreover, I think not mixing fats and carbs might lower hedonism too. Not that I think they don't enjoy their food.
I agree that salted food tastes over-salted after a period of reduced salt intake. Most fruitarians I know of don’t use salt, however, they (true fruitarians, not low-fat raw vegans/80/10/10ers) will mix carbs and fat and eat durian. For the first 3 years of fruitarianism I didn't use salt, but by the 4th year I used it liberally after developing anxiety attacks that went away when I started salting my food again.
I think disproportionately high focus on health research is induced by the diseased state and I can totally believe that it's a relief when you are successfully able to let it go! That's not what life is really about after all. But that's also a sign that you are not in a learned helplessness state.
Agreed. That's definitely not what life is really about.
I'll try it soon and report it
I look forward to reading about your experience with it.
-
@Amazoniac said in cancer:
If you've been moved by respect, feel free to ignore the posts.
Thank you.
Jennifer,
I'm the one to thank you for clarifying that you weren't invested on this to defend your views, but out of respect for the conversation. After all, it would take disrespects at any moment to avoid being intensely argumentative. An unbearable one:
- 'I would prefer not to discuss this topic further, will refrain from commenting for now, and hope that you don't mind.'
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login