Conditional problems with vitamin A: a place for sane discussions
-
Cyclosporine is also an effective treatment for psoriasis. Given the extensive evidence of vitamin A’s role in immune function, I think it is more likely that psoriasis improvement with a depleting diet is a side effect of immune suppression instead of a root cause being discovered.
https://pubmed.ncbi.nlm.nih.gov/11375434
“Vitamin A deficiency impairs innate immunity by impeding normal regeneration of mucosal barriers damaged by infection, and by diminishing the function of neutrophils, macrophages, and natural killer cells. Vitamin A is also required for adaptive immunity and plays a role in the development of T both-helper (Th) cells and B-cells. In particular, vitamin A deficiency diminishes antibody-mediated responses directed by Th2 cells, although some aspects of Th1-mediated immunity are also diminished.”
-
It directs to..
a) Professor Smith:
"If a person takes in more toxic "vit" A than they excrete on a regular basis, then they are ACCUMULATING it in their liver and bodyfat
If 306 mcg beta-carotene (that's 1020 IU, one carrot has 6000 IU!) took 58 DAYS to turn over...do you realize just how fast you are filling up with this toxin?
1 beta-carotene eventually has to split into 2 retinaldehydes"
b) Disciple:
"Wow.
And this is also a great study for showing how much beta-carotene is actually converted to retinol. They write a minimum of 62% is turned into retinol. So a lot will eventually go the retinol route.
"What is clear is that, by our estimates, a minimum of 62% of the absorbed β-carotene was cleaved to vitamin A and by this reasoning the vitamin A value of β-carotene dose was 0.53. [The calculation is as follows: Assuming central cleavage, 1 mol of β-carotene yields 2 mol of vitamin A. If 62% of the absorbed β-carotene were cleaved to vitamin A, 1 mol of β-carotene would yield 1.24 mol of vitamin A. Thus, the vitamin A value of the absorbed dose is 1.24. Yet, the dose was 42.6% absorbed. So, the actual vitamin A value is (1.24) (0.426) or 0.53.]"
1 molecule of beta-carotene turns into 2 molecules of "active vitamin A".
The 0.53 value means that 1mg of ingested beta-carotene will turn into 0.5mg retinol. In other words, one medium carrot (eaten with lots of fat) can be equivalent to 27g beef liver.
Due to the time-delayed conversion, an acute poisoning is not possible, but a chronic poisoning is."
Their claims:
- a) "[..]one carrot has 6000 IU!" (1,800 mcg)
- b) "[..]one medium carrot (eaten with lots of fat) can be equivalent to 27g beef liver."
Beef liver:
- Poisonol 10,000 mcg/100 g
Carrot:
- Alpha-carotene: 2,000 mcg/carrot
- Beta-carotene: 5,000 mcg/carrot
We can disconsider half of the alpha-carotene amount and treat the other half as beta-carotene:
Beef liver:
- Poisonol 10,000 mcg/100 g
Carrot:
- Beta-carotene: 6,000 mcg/carrot
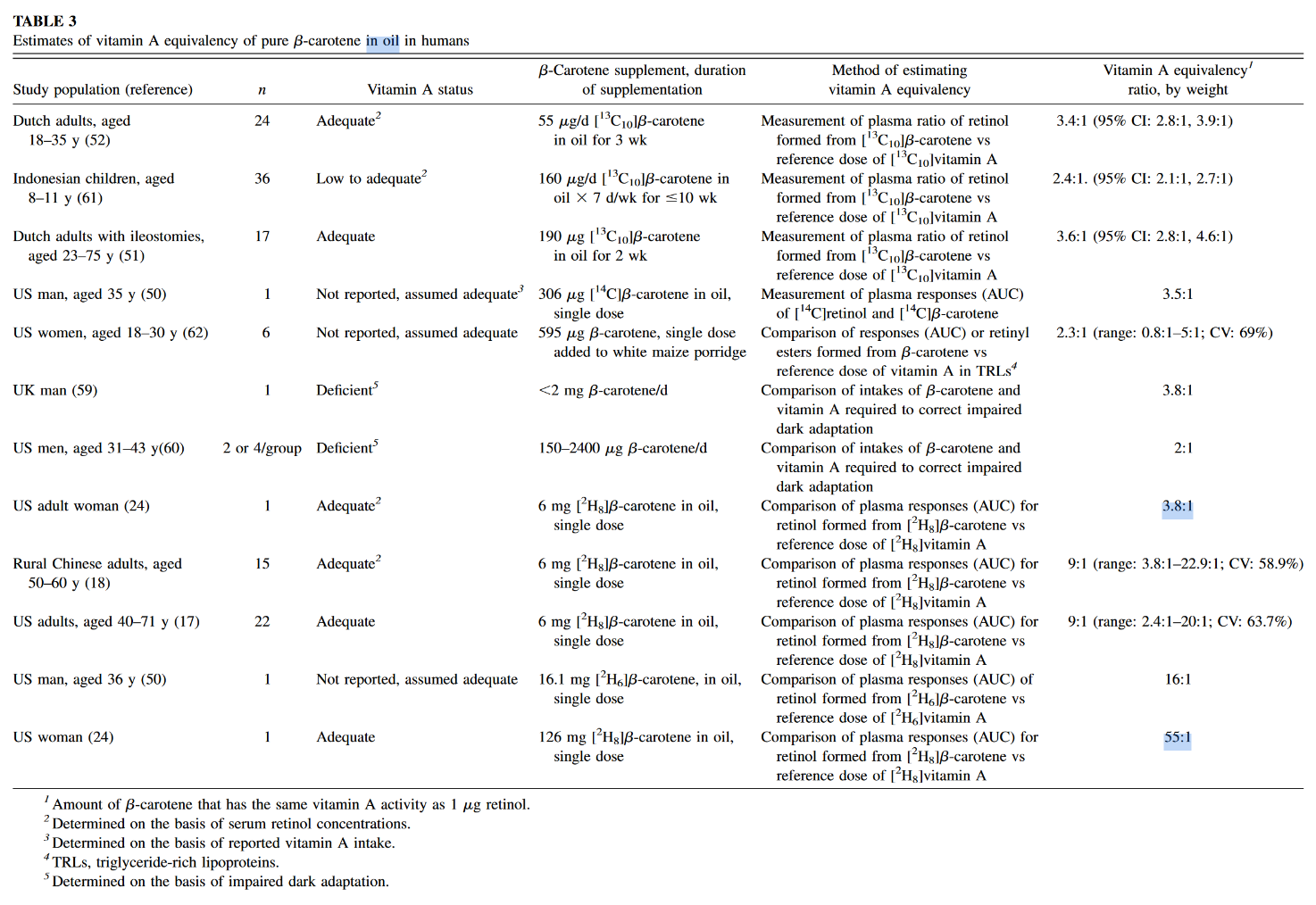
The author of the second post seems to be into the topic of poison A for a while, yet for some reason acts as if the information presented in the mentioned experiment was novel. These equivalences are found in almost all textbooks, even the main sections of the dedicated Wikipedia page have them, suggesting that pure b-macabrotene has half of the activity of poisonol:
- 1 µg RAE = 1 µg retinol from food or supplements
- 1 µg RAE = 2 µg all-trans-β-carotene from supplements
Now the equivalences from their claims:
- a) 1 µg RAE = 3.3 µg of all-trans-β-carotene from carrots
- b) 1 µg RAE = 2 µg of all-trans-β-carotene from carrots
The disciple is basing his equivalence on the following values from the linked experiment:
- Absorption: 42.6%
- Conversion: 62%
- Total (42.6% × 62%): 26%
This is close to a quarter, that results in a mass equivalence of about poison 1:4 b-mac, not 1:2 as he's arguing.
The source of confusion is because he's applying a molar to a mass ratio. B-carotene can yield two poisonols, but the mass is going to remain similar after cleavage and metabolism, with minor gains from the incorporation of new elements (that I'm going to disregard).
To arrive on his value:
- 26% × 2 = 53% (0.53)
It would've been preferable for the disciple to state:
"The 0.53 value means that 1 mg of ingested beta-carotene will turn into
0.5mg~0.25 mg retinol." The factor accounted for the potential of b-carotene to yield two poisonols, so it has to be applied after we halve the amount.At this stage, we can already discard the idea that a carrot will poison you as an ounce beef liver.
The spinach used in the quoted experiment served to tag macabrotene, the plant assimilated the labeled carbon of CO2 from the environment, allowing them to track the poison. But when it was time to contaminate the victim, the macabrotene was isolated and given in purified form at a low dose.
The food matrix lowers the availability of toxins, making them more difficult to be extracted, which is why researchers define a marked drop in efficiency when the b-macabrotene is derived from foods:
- 1 µg RAE = 1 µg retinol from food or supplements
- 1 µg RAE = 2 µg all-trans-β-carotene from supplements
- 1 µg RAE = 12 µg of all-trans-β-carotene from food
If we ignore this factor and pretend that fibrous carrots are an oil, the amount used in the experiment was modest (300 mcg) and we know that the rate of absorption and conversion tends to decrease as the dose gets high.
But let's reject this too and assume that it remains uninhibited up to 6 mg or so. However, the adjustment is beyond the meal content, the degree of body contamination with the poison is another factor that determines its fate. It's why the purity of the victim matters to interpret the dosing response to carotenoids: contaminated and decontaminated persons will metabolize it differently. When the body is overloaded, the rate of conversion to retinoids is reduced. To a lesser extent, the same goes for their absorption. Yet, carotenoids can be excreted intact.
"1 beta-carotene eventually has to split into 2 retinaldehydes"
It doesn't. His own equivalence conflicts with this claim, even if we discount the unabsorbed fraction (and he probably didn't):
"1 beta-carotene eventually has to split into 2 retinaldehydes":
- 6,000 mcg b-carotene → about 6,000 mcg PAE
"1 [absorbed] beta-carotene eventually has to split into 2 retinaldehydes":
- 6,000 mcg b-carotene → about 2,500 mcg PAE
"[..]one carrot has 6000 IU!":
- 6,000 mcg b-carotene → about 1,800 mcg PAE
Which is it?
"If you take something more than you can excrete, you accumulate"
Of course.
"If 306 mcg beta-carotene (that's 1020 IU, one carrot has 6000 IU!) took 58 DAYS to turn over...do you realize just how fast you are filling up with this toxin?"
A long half-life doesn't result in an indefinite accumulation, only until a steady state is reached, when poisoning for profits should plateau with regular consumption. Something like this in dosing more often:
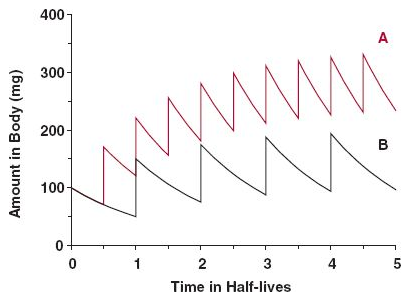
Source: the internet.Some accumulation is normal and healthy; or should we treat macabrotenoids as toxins to be nuked from the body at all costs? "Vitamin" E is a toxin too (Smith, 2023), but is it harmful when it's not detoxified fast enough to avoid a detectable level, leading to 'accumulation' to be associated with problems?
Consider this: you consume a meal, whose elimination would take 24 hours. Instead of waiting for this period to eat the next, you consume multiple meals in between (may be 4 in a day), that result in accumulation of matter, but without issues. The accumulation is temporary, purposeful and the body is adapted to it. It's not immediate, but the matter eventually leaves the body to the extent that it's consumed: no stuffing until explosion occurs because the input matches the output despite the delay.
Excess carotenoids or calories should come with signs. The early stages are benign, will indicate that the person has to cut back or improve the capacity to handle them. Yet, carotenemia isn't reliable to diagnose poison A toxicity because it can be caused for different reasons (such as lack of nutrients or poor protein synthesis). As an example, if a person needs to take supplemental thyroid hormones and suddenly stops the treatment, it can be followed by carotenemia.
The rate of storage and mobilization is adaptable as well. In case someone discontinues the consumption of poisons altogether, it can signal conservation and a longer persistence in the body. Therefore, the length is variable.
All in all, while we have people debating whether an inability to convert macabrotenes is common or a real concern for persons who don't consume preformed poisons, we have the poison A crowd alarming you that regular carrot consumption is a ticket to the hospital over time, for having the same potential of destruction as liver in the diet, neglecting the multiple steps that regulate these toxins as drugs. #toxicbileapocalypse
-
Gut commensals expand vitamin A metabolic capacity of the mammalian host
"Here, using liquid chromatography-tandem mass spectrometry (LC-MS/MS), we found that the presence of commensal bacteria resulted in a high concentration of the active retinoids, atRA and 13cisRA, as well as the principal circulating retinoid, ROL in the mouse gut lumen. Our work demonstrating gut bacteria’s VA metabolic capacity in generating multiple pharmacologically active retinoids lays the groundwork for developing bacterial retinoid therapy to treat diseases and tackle VA deficiency disorders."
"Cecum was chosen since it harbors the largest consortia of metabolically active bacteria in the digestive tract. To obtain a precise snapshot of flux in VA metabolites due to gut microbiome intrinsic VA metabolic activity, we compared the retinoid metabolomes from cecal contents from germ-free (GF), conventional (CV), and antibiotic treated mice (CV+Abx)."
"We saw that the cecal contents of GF mice had significantly lower concentrations of atROL, atRA, and 13cisRA compared to CV mice cecal contents (Figures 1B–D). This pattern was also observed along the length of the intestine (
Figures S1A–G). The observed differences in VA metabolites were not due to differences in dietary RE since both the GF and CV mice were maintained on similar autoclavable diet and had equal levels of dietary retinyl palmitate in their cecal contents (Figure 1E). Importantly, CV mice treated with cocktail of antibiotics in drinking water for 3 days showed drastic depletion in concentrations of all VA metabolites except for RE in the cecal contents compared to the control mice (Figures 1B–E), establishing that the presence of gut microbiome is required for high amounts of ROL, atRA and 13cisRA in the gut lumen. Taken together, our data suggest that members of the gut microbiome have the metabolic potential to process dietary VA into ROL and generate its active metabolites atRA and 13cisRA."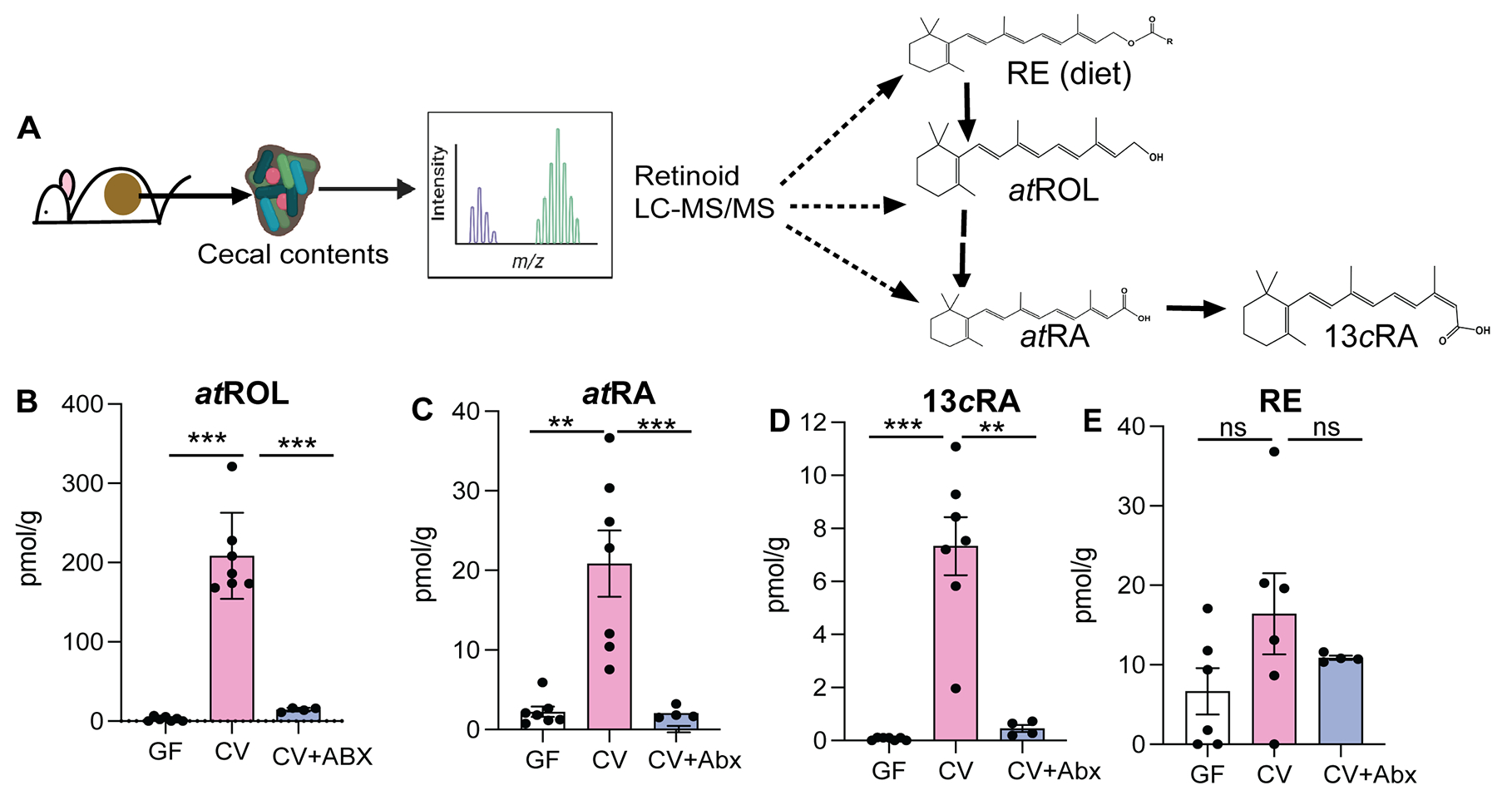
"Next, we investigated if VA metabolic activity observed in the gut lumen was correlated with presence of specific bacterial members. To determine the VA metabolic potential of different bacterial groups, CV mice were treated with either
- Vancomycin, which targets anaerobic commensals belonging to class Clostridia and Bacteroidia (Duncan et al., 2021), or
- Neomycin, which specifically targets aerobic commensals such as Proteobacteria (Hazenberg et al., 1983).
We observed that vancomycin treated mice had significantly lower ROL, atRA and 13cisRA concentrations in the gut lumen compared to untreated mice (
Figures 2A–C). Neomycin treatment did not affect retinoid levels in the gut lumen. The reduction in retinoids in the gut lumen of vancomycin treated mice was not due to reduced bacterial load (Figure S2C) suggesting that vancomycin sensitive commensal anaerobes provide the VA metabolic activity in the gut lumen.""To confirm the differential ability of commensal bacteria to metabolize VA, we colonized GF mice with Proteobacteria that bloom during vancomycin treatment (
Figure 2D). A second group of GF mice were given Clostridia spores in addition to Proteobacteria isolated from vancomycin treated mice. GF mice colonized with Proteobacteria alone did not show any increase and had comparable amounts of retinoids in the gut lumen as GF controls (Figures 2E–G). In contrast GF mice colonized with Proteobacteria and Clostridia spores showed significant increase in concentrations of atROL, atRA and 13cisRA in the gut lumen. 16S rRNA analysis of cecal community confirmed that gut microbiomes of Proteobacteria colonized mice lacked commensal anaerobes while mice that received spores in addition to Proteobacteria had high abundance of bacteria belonging to class Clostridia that restored all three retinoids in the gut lumen (Figure 2H).""We previously showed that gut bacteria can modulate VA metabolic machinery in the IECs and regulate RA amounts in intestinal tissue (Grizotte-Lake et al., 2018). To establish that bacteria intrinsic VA metabolic activity in the gut lumen is independent of host VA metabolic machinery, cecal contents from CV mice were harvested and grown in nutrients rich media and then supplemented with 10mM RE or ROL under anaerobic conditions. After 3 hrs., conversion of VA precursors into ROL, atRA and 13cisRA was quantified by LC-MS/MS (
Figure 3A). In the presence of bacteria, RE was hydrolyzed into ROL and ROL was oxidized to RA isomers (Figures 3B–F and S3). Bacterial cultures by themselves did not contain any detectable ROL or RE. The media alone supplemented with RE, or ROL did not yield quantifiable metabolites (Figures 3B–F) suggesting that there was no spontaneous conversion of RE and ROL into RA. These results establish that cecal bacteria can metabolize dietary VA precursors to active metabolites independent of the mammalian hosts and that gut bacteria encode the genetic machinery needed for performing VA metabolism." "Taken together, our results demonstrate that culturable consortia of gut bacteria can perform all the enzymatic reactions required for VA metabolism generating retinoid metabolites independently of the host.""Many Lactobacillus spp are naturally resistant to vancomycin (Swenson et al., 1990), and accordingly we observe that vancomycin treatment can result in bloom of Lactobacillus spp (
Figure S2B). We found that L. intestinalis, which has high ALDH activity was highly sensitive to vancomycin (Figure S4B) suggesting that loss of L. intestinalis upon vancomycin treatment could result in reduced retinoid metabolites in the gut. To evaluate if probiotic application of L. intestinalis to mice during vancomycin treatment would restore RA levels in the gut, mice were treated for 10 days with vancomycin and were given three applications of 108 CFUs of L. intestinalis or L. murinus. Similar bacterial loads were observed in all groups (Figure S4C). Retinoid analysis showed that L. intestinalis restored atRA levels of vancomycin treated mice while L. murinus, that does not show ALDH activity could not restore gut RA levels in vancomycin treated mice (Figure 4F)."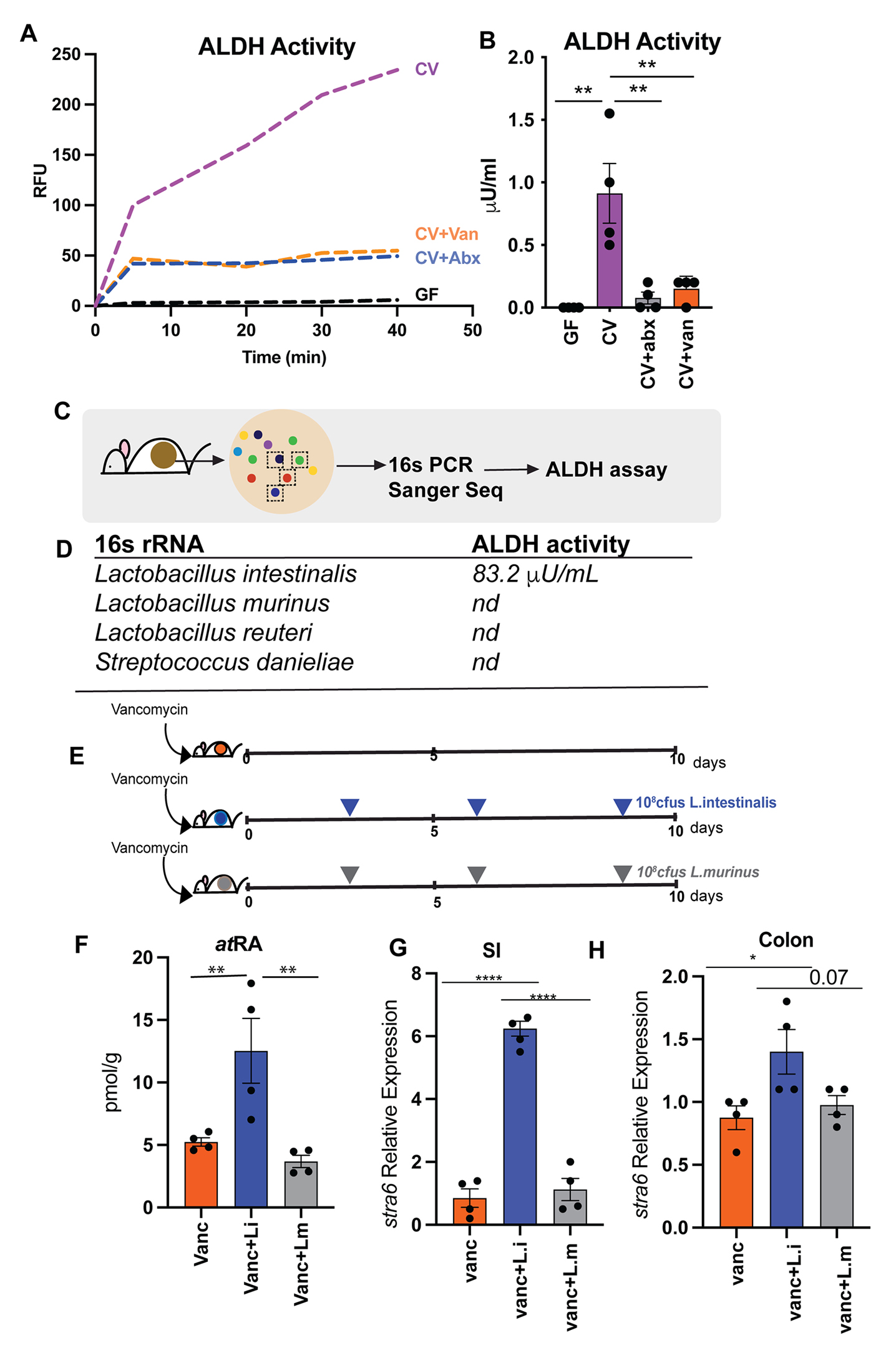
"[..]monocolonization of GF mice with either L. intestinalis, SFB or B. bifidum did not restore RA levels in the gut of GF mice (
Figure S4A) indicating that VA metabolism is an emergent property of gut microbiome and requires other members of consortia to participate in multistep conversion of VA to RA. In vancomycin treated animals L.intestinalis is able to restore RA production due to presence of vancomycin resistant bacteria that provide the metabolic machinery needed for other steps of VA metabolic pathway.""Next, we wanted to determine if restoration of RA in gut lumen following L. intestinalis treatment would induce RA responsive genes in the host. To do this we quantified known RA inducible host gene, Stra6 (Carrera et al., 2013; Kawaguchi et al., 2007). STRA6, has been shown to be essential in facilitating the cellular entry and exit of retinol and therefore is key in regulating how much retinol host cell can uptake. RA inducible gene stra6 was significantly induced in small intestine and colon of L. intestinalis supplemented mice compared to non-supplemented and mice gavaged with L. murinis (Figures 4G–H). We also observed higher expression of Nos2 gene [iNOS] in small intestine of the L. intestinalis supplemented mice in comparison to non-treated and L. murinis supplemented mice (
Figure S4D). The nitric oxide synthase 2 (nos2) gene was recently shown to be inducible by bacteria derived RA in the intestinal epithelium and its upregulation protected against pathogen colonization (Woo et al., 2021). We did not detect any significant differences in the pattern of inflammatory cytokines expressions in the small intestine and colon between the groups (Figures S4E–F) suggesting that addition of L. intestinalis is not linked to inflammation. Overall, our results demonstrate that bacteria with ALDH activity can restore RA following its depletion upon antibiotic treatment and promote the induction of RA responsive genes in the host." -
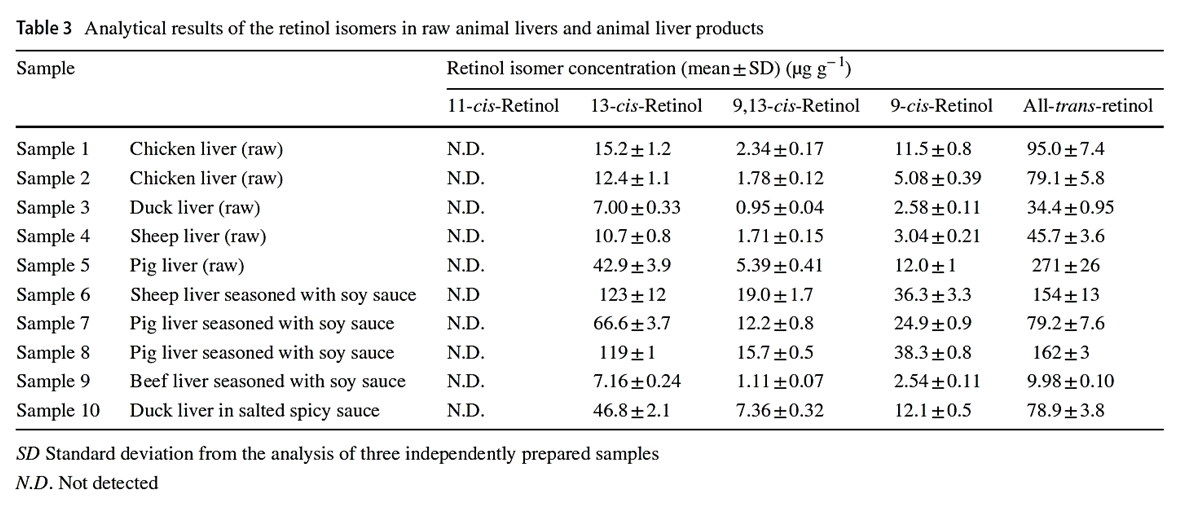
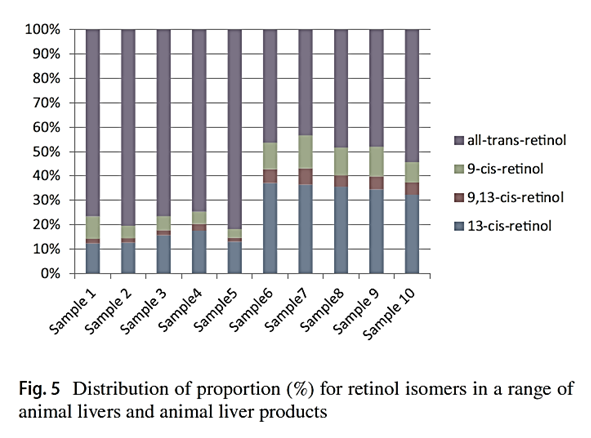
"Considering that the biological activities of isomers are lower than all-trans-retinol, the knowledge of retinol isomer profile in liver is useful for a precise estimation of safe dietary intake levels of animal liver."
"[..]when the determination can not separate retinol isomers, total retinol activity in animal liver products may be overestimated."
-
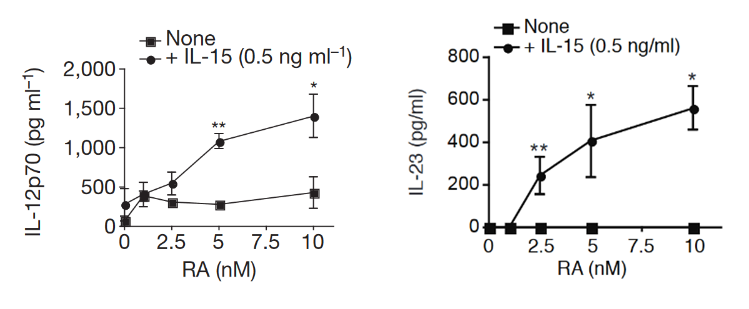
Co-adjuvant effects of retinoic acid and IL-15 induce inflammatory immunity to dietary antigens
"Here we find in mice that in conjunction with IL-15, a cytokine greatly upregulated in the gut of coeliac disease patients[3,7], poisonoic acid rapidly activates dendritic cells to induce JNK (also known as MAPK8) phosphorylation and release the proinflammatory cytokines IL-12p70 and IL-23."
"Our study reveals that in the presence of IL-15, RA has unforeseen co-adjuvant properties that induce TH1 immunity to fed antigens (
Fig. 4f). It indicates further that under infectious conditions associated with induction of IL-15 and IL-6 in the intestinal mucosa, RA will also promote TH17 immunity. These observations caution against the use of poison A and RA for the treatment of autoimmunity and inflammatory intestinal disorders associated with high levels of IL-15. Indeed, a causal relationship between retinoids used for the treatment of acne and inflammatory bowel disease has been implicated in a subset of patients[25].""More generally, our study supports the concept that there are no ‘unconditional’ suppressive factors, and that integration of tissue and exogenous signals determine the class of the immune response, which ultimately needs to be tailored to the tissue and the antigen. In line with the idea that the same proinflammatory factors trigger different immunological outcomes depending on the tissue in which they are induced, we found that the ability of IL-12 to inhibit Treg-cell induction was blocked by butyrate, a metabolite produced by commensal bacteria present in the colon but not in the small bowel (data not shown)."
"Our observations may also explain why oral tolerance is disrupted in patients with inflammatory bowel disease[28] who also have dysregulated IL-15 expression in the gut[29]. Lastly, our results indicate that inhibiting IL-15 signalling may constitute a therapeutic intervention to restore mucosal tolerance to luminal antigens."
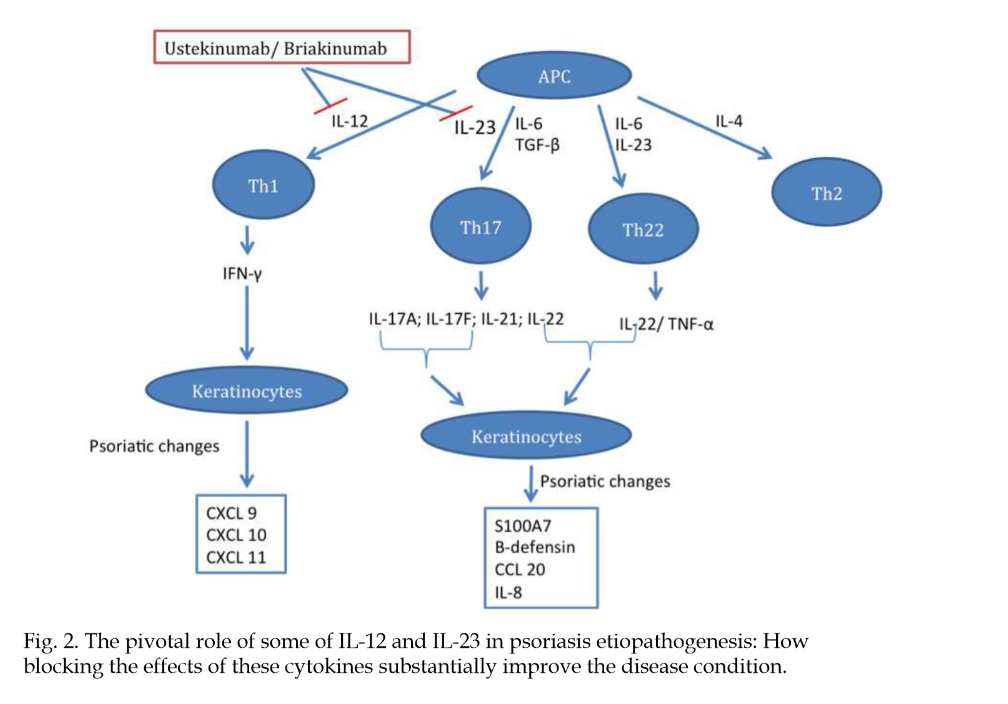
Insights into the Pathogenesis and Treatment of Psoriasis
"[..]dendritic cells and effector T-cells are important in the development of the psoriastic lesion, and cytokines produced by these cells stimulate keratinocytes to proliferate and increase the migration of inflammatory cells into the skin, promoting epidermal hyperplasia and inflammation (Monteleone, G. et al., 2011)."
"An increase in efficacy and reduction of adverse events are the main drivers for new therapies. Infections, one type of adverse event, usually increase in patients receiving anti-cytokine therapy (Dinarello, 2003)."
"Some inflammatory agents, whether physical, chemical, or infectious, induce an intense immune response. This immune response against them frequently results in tissue damage that could be more intense if it were not for the interference of regulatory mechanisms (Belkaid et al., 2006). As has already been specified, Treg cells help limit the damage caused by a vigorous immune response."
"Similarly, excessive activity of Treg cells may limit the magnitude of the immune response, which may result in failure to control an infection. On the other hand, the absence of the T regulator may result in intense inflammation and autoimmune dermatitis. Tissue damage may also result from the development of effector cells against their own auto-antigens (Figure 4)."
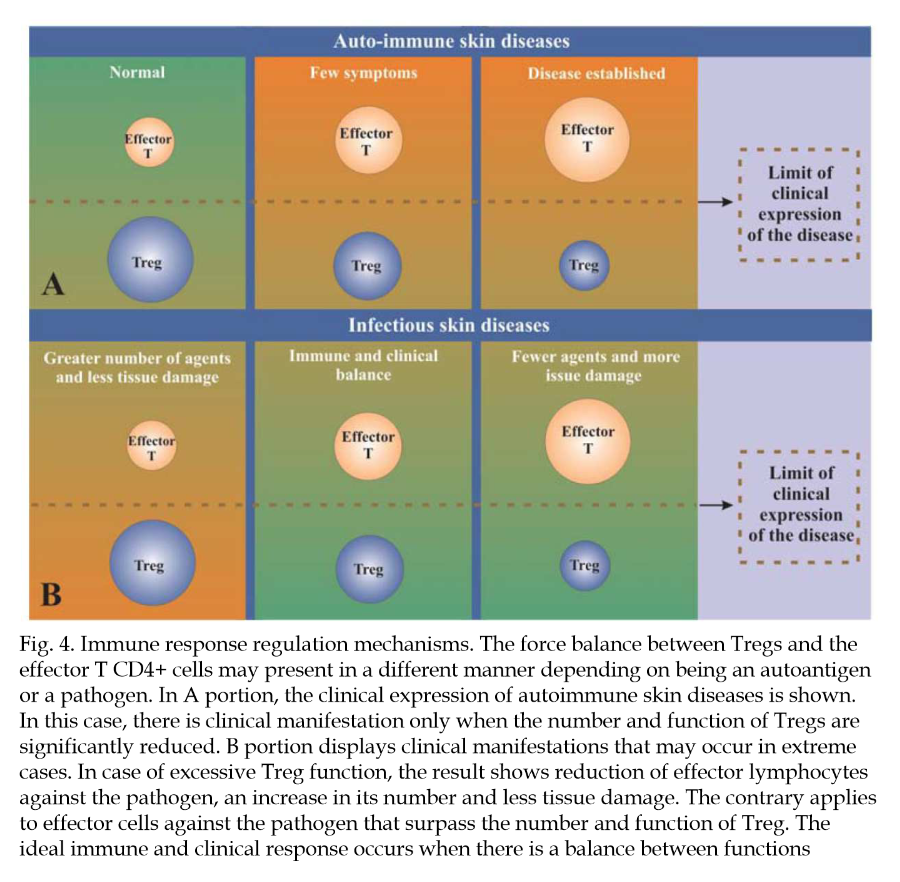
"An improved understanding of the role of T regulators in psoriasis may lead to the identification of new targets for treatment. More specifically, the goal is to manipulate natural regulator cells or those induced by means of an increase or decrease of their function, depending on the circumstances."
Immunopathogenesis of inflammatory bowel disease
"Altered gut permeability may lead to increased bacteria adherence and inappropriate exposure of the mucosal immune system to bacterial products causing inflammation."
"Negative regulation of the host innate immune responses to the indigenous microflora maintains gut homeostasis. Key players in the negative mucosal regulation include interleukin-10 (IL-10) and IL-2, as evidenced by mice with deficiencies in these factors develop spontaneous intestinal inflammation, but are protected from intestinal disease when raised in germ-free environments[77–>79]. This indicates that at steady state, pathologic consequences of immune activation by commensal microflora are constitutively inhibited by IL-10 and -2 dependent mechanisms."
"A subset of T cells producing IL-6 and IL-17, now known as Th17 cells, has emerged as an important mediator of the T-cell response in gut inflammation (Figure 4)."
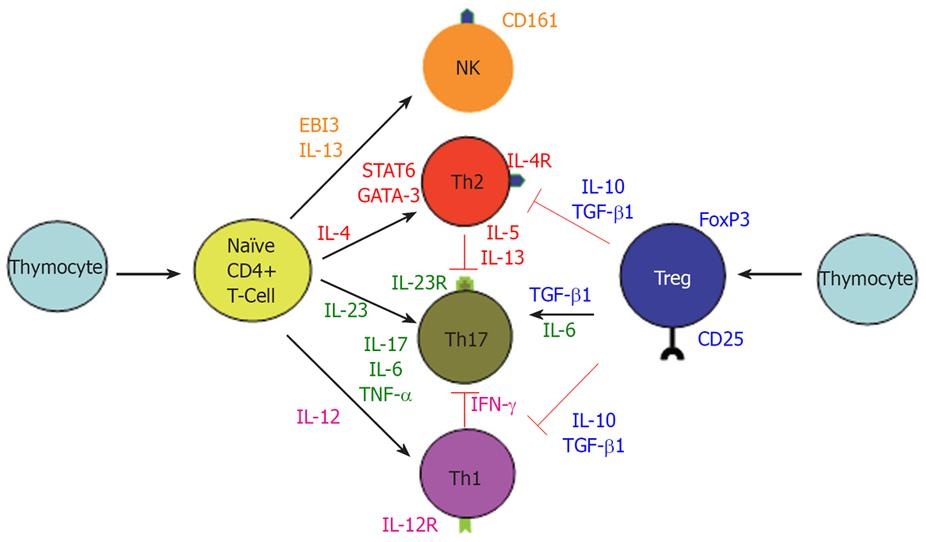
"The above findings do not exclude the role of exaggerated Th1 response in CD since IL-12/IFN-γ and IL-23/IL-17 may be parallel pathways involved in inflammatory response. Interestingly, IL-12/IFN-γ and IL-23/IL17 pathways are mutually exclusive, since IFN-γ suppress IL-17 and vice versa (Figure 4)[104]. It is of pathogenic importance to consider all of the major immune pathways that are responsible for the development of CD. For example, therapeutic targeting of only the newly discovered IL-23/IL-17 immune axis may actually exacerbate CD by accelerating the IL-2/IFN-γ Th1 pathway."
-
@Amazoniac
I hope others will contribute to this thread re absorption and clearance rates as well as mechanisms by which vit A may be poisonous/problematic. Are you personally limiting vit A intake at this time?I’m not (yet). Given what’s going on at RPF, I have, if anything upped eggs/milk/pumpkin/etc in my diet over the last few months to celebrate high-metabolic-rate good health, Ray Peat style, as quiet dissent. Like Amazoniac, I think it’s good for us to remain open to new information as it arises, however, about any potential problems associated with excessive vit A intake.
Might I get your advice based on my brief personal history, which was unusually high-dose vit A for several reasons? Growing up in the 1970s, my mom became a health-food nut and both mom and dad took – and gave me as a child – a large volume of vitamin supplements. From the age of 3 onwards (maybe through puberty), I was encouraged to take a daily beta-carotene supplement. We drank lots of carrot juice. The soles of my feet had an orange tint, which my doc may have even commented on once. We kept up this extraordinarily high diet + supplement regimen until I was a teenager. I took a round or two of Accutane for acne as a 17 year old. Under lots of other stressors and chronic sleep deprivation, I was diagnosed as a type-1 diabetic at age 20, which ran in my half-Norwegian family. I would be a likely candidate to have had – and very likely still have – excessive vit A stored in liver, adipose and elsewhere. Do you think I should try the low vit-A diet? (I can’t believe I’m actually writing those words…!!!...rest assured, only as a speculative hypothesis and not a likely action plan.)
-
@T-3
Adding: I never had (and don't think I have at present) any vit A toxicity symptoms. The callouses on my feet and palms are probably a bit more "orange tinted" than most people's and my complexion is noticeably darker than either of my parents, but I also get a lot of healthy sun exposure. My default is skepticism toward the hypothesis that I suffer from vit A toxicity. Eating high-vit-A foods makes me feel good and I don't think I have any problems associated with those foods. Thus, I'd say that worrying about vit A intake would be creating a pseudo diet problem where none in fact exists. But I gather that Amazoniac has made this thread because he has some concerns about vit A in his own diet, or is that wrong? -
https://www.bioenergetic.life/clips/8442a?t=813&c=17
"So a lot of these oils that are purported to be good for our health are actually quite thyroid toxic and long-term use could lead to conditions that are common in low thyroid and is as detrimental as cancer. Yeah. And there's one which isn't really a fatty acid, but it's a highly unsaturated molecule, carotene, which is the precursor to vitamin A. It not only blocks the cellular sites that use vitamin A, but as a polyunsaturated molecule, it also blocks the thyroid function every place that the vegetable oils do."
-
@DavidPS Thanks for posting this quote from Ray. Apropos! DavidPS, are you limiting eggs, oranges, persimmons, pumpkin, sweet potato and the like?
Is the retinol in milk different from the beta carotene in orange colored foods?
I think I'm asking embarrassingly basic questions here. And I worry my advice request may inadvertently be derailing what Amazoniac wanted this thread to be about. I just wanted to get expert advice re practical take-aways from those of you thinking carefully about the evidence base from published studies regarding risks of excessive retinol and/or beta-carotene-containing foods. Has what you've learned about vit-A risk changed the way you eat?
-
Most here are familiar with RP's discovery that a daily carrot salad made him feel better. Some think it was because of the "colon sweeping" effect, but if that were the case, wouldn't charcoal have the same effect? Could it be because Beta carotene is an effective modulator of the gut biome?
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10220829/
-
@S-Holmes
-
@T-3 - Thanks for your kind words. I am trying to make sense of it all. Danny Roddy helped me understand that vitamin A is essential (that why it is a vitamin) and has a recent video (3 minutes) that discusses its role making hormones in the body.
In addition, Dr Peat wrote in his article, BSE - mad cow - scrapie, etc.: Stimulated amyloid degeneration and the toxic fats:
"The amyloidoses affect different tissues in different ways, but when they occur in the brain, they produce progressive loss of function, with the type of protein forming the fibrils determining the nature of the functional loss. The protein which carries thyroid hormone and vitamin A, transthyretin, can produce nerve and brain amyloid disease, but it can also protect against other amyloid brain diseases; in Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and the “prion diseases” (scrapie, kuru, CJD, BSE, etc.) amyloid particles are formed by different proteins. The transthyretin protein which is binding small molecules resists condensation into the amyloid fibrils, but without its normal vitamin A and thyroid hormone, it can create toxic fibrils. (Raghu, et al., 2002.)"
I found that passage to be scary. One does not want to go too low in vitamin A. I get mine from real foods and I do not limit my consumption based on vitamin A. I do not use vitamin A supplements and topical A may be counterproductive.
Enhancement of chemical carcinogenesis in the hamster cheek pouch by prior topical application of vitamin A palmitate -
@S-Holmes said in Conditional problems with vitamin A: a place for sane discussions:
Most here are familiar with RP's discovery that a daily carrot salad made him feel better. Some think it was because of the "colon sweeping" effect, but if that were the case, wouldn't charcoal have the same effect? Could it be because Beta carotene is an effective modulator of the gut biome?
I can share, anecdotally, that carrot salad always helps me, charcoal does not, with regard to transit time and moving the train down the tracks. I believe the carrot salad's effectiveness is due to the mere mechanics of the fibrous carrot moving through your system. At least that is how it feels to me.
-
@T-3 said in Conditional problems with vitamin A: a place for sane discussions:
@Amazoniac
I hope others will contribute to this thread re absorption and clearance rates as well as mechanisms by which vit A may be poisonous/problematic. Are you personally limiting vit A intake at this time?I’m not (yet). Given what’s going on at RPF, I have, if anything upped eggs/milk/pumpkin/etc in my diet over the last few months to celebrate high-metabolic-rate good health, Ray Peat style, as quiet dissent. Like Amazoniac, I think it’s good for us to remain open to new information as it arises, however, about any potential problems associated with excessive vit A intake.
Might I get your advice based on my brief personal history, which was unusually high-dose vit A for several reasons? Growing up in the 1970s, my mom became a health-food nut and both mom and dad took – and gave me as a child – a large volume of vitamin supplements. From the age of 3 onwards (maybe through puberty), I was encouraged to take a daily beta-carotene supplement. We drank lots of carrot juice. The soles of my feet had an orange tint, which my doc may have even commented on once. We kept up this extraordinarily high diet + supplement regimen until I was a teenager. I took a round or two of Accutane for acne as a 17 year old. Under lots of other stressors and chronic sleep deprivation, I was diagnosed as a type-1 diabetic at age 20, which ran in my half-Norwegian family. I would be a likely candidate to have had – and very likely still have – excessive vit A stored in liver, adipose and elsewhere. Do you think I should try the low vit-A diet? (I can’t believe I’m actually writing those words…!!!...rest assured, only as a speculative hypothesis and not a likely action plan.)
@T-3 said in Conditional problems with vitamin A: a place for sane discussions:
@T-3
Adding: I never had (and don't think I have at present) any vit A toxicity symptoms. The callouses on my feet and palms are probably a bit more "orange tinted" than most people's and my complexion is noticeably darker than either of my parents, but I also get a lot of healthy sun exposure. My default is skepticism toward the hypothesis that I suffer from vit A toxicity. Eating high-vit-A foods makes me feel good and I don't think I have any problems associated with those foods. Thus, I'd say that worrying about vit A intake would be creating a pseudo diet problem where none in fact exists. But I gather that Amazoniac has made this thread because he has some concerns about vit A in his own diet, or is that wrong?The terms 'macabrotenoids' and 'poisonoids' are for fun. It used to be clear early on, but the poison A crowd took the confusion to proportions that may create doubt for some people on whether these are humorous or not.
You can find a report (on the main poison A thread of the Garrey Smeat Forum) from researchers who found that people with diabetes and hypothyroidism were groups that had unusually elevated stores of poisonol. What increases the metabolic rate tends to also increase the internal consumption of poison A, and reserves can be normalized this way rather than through restriction.
I think that the community has to separate excess poison A stores from its toxicity. Lumping them invariably together contributes to the pro-poison A and
anti-poison Apro-life camps going on futile debates.The person doesn't have to be overloaded with poison A in the body to experience toxicity problems, these can happen at low intakes when the metabolism of a substance is deranged or if its addition influences pathways that are maladjusted (⇈).
And we don't know when it's really a maladjustement, making avoidance risky. The elevation of poisonoids may be containing an infection or inhibiting cancer. If the immune system is suppressed, it can represent easing on a battle, forcing the body to find ways to internalize the problem and minimize the associated cost.
One of the sources of poison in the gut is what recirculates through bile, that may contribute to local problems as dietary poisons do, but what's framed as 'detoxification events' can be the body transitioning from aggressive mode to tolerance. Something of this nature would align with people suddenly being able to not overreact to foods that used to cause trouble.
In the previous post, the authors pointed out that inhibition of specific inflammatory proteins carries risks (despite improvements). I suppose that it's riskier to try to inhibit inflammation manipulating at a more basic level through poison A restriction.
Poison A deprivation is a desperate immunosuppressive measure and doesn't seem to apply to your case. And you already mentioned to respond well to contaminated foods. So, I wouldn't bother with it.
If the body has an overactive pathway, any fluctuation in the availability of a precursor can result in exaggerated formation of derivatives. An example of this would be someone with sarcoidosis, who may have a shock-like response to small amounts of venom D3 because of excess conversion to metabolites that are more active. It's toxicity at low doses without the person being overloaded with venom in the body. When someone treats it as rat poison, it can be that for this individual it's behaving as such: a poison to a rat. It's converted in excess, that would normally take much higher doses of the precursor to achieve the same effect. The poison A crowd tend to have poor tolerance to venom D3 as well, and exposure to toxins should be regulated as drugs.
Unrelated:
- Control by the brain of vitamin A homeostasis (it's not about the abdominal brain, but the intracranial one)
-
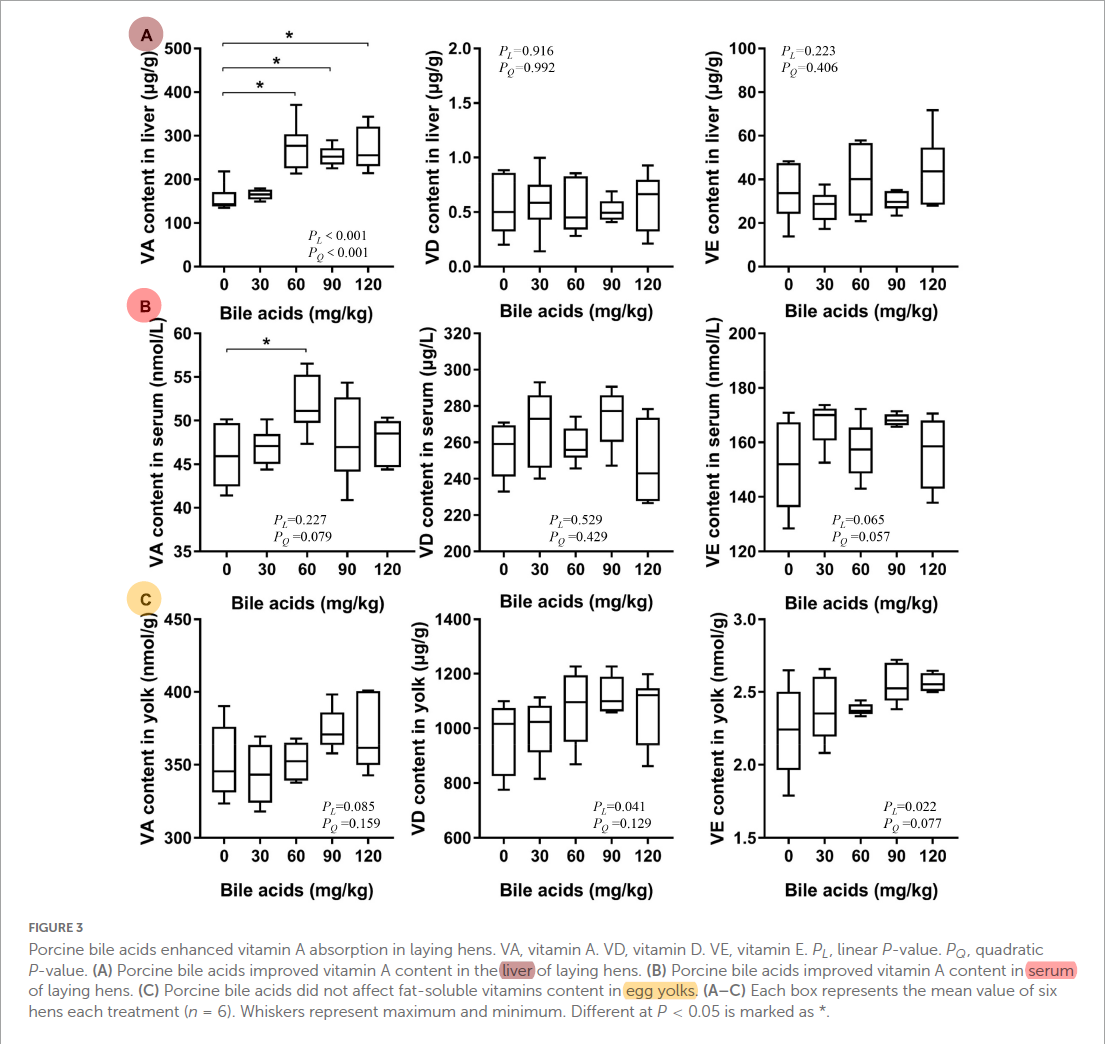
Porcine bile acids promote the utilization of fat and vitamin A under low-fat diets
"Hens were randomly divided into five treatment groups with six replicates of 15 birds per replicate. The five treatment groups were fed with: corn soybean meal diets supplemented with 0, 30, 60, 90, and 120 mg/kg porcine BAs, respectively. No extra fat was added to the basic diet (crude fat was 3.23%). The whole experimental period was 84 days, and the pre-feeding period was 7 days."
"The porcine BAs are composed of the following components: 7.99% of hyocholic acid, 19.65% of chenodeoxycholic acid, and 70.88% of hyodeoxycholic acid."
"In vivo, different kinds of fat-soluble vitamins are absorbed at different sites. For example, vitamin A is mainly absorbed in the proximal intestine, while vitamin D is absorbed in the median intestine and vitamin E is absorbed in the distal intestine (49). The preferential absorption of vitamin A competes against the absorption of other fat-soluble vitamins (49)."
"[..]supplementation of BAs in the diet of laying hens resulted in an increase in the content of vitamin A in the liver ["by 60-75%"], while vitamin D and E did not change significantly in the in vivo experiments."
"The present study concluded that BAs promoted the absorption of vitamin A by promoting the absorption of fat even under low-fat diets, thereupon improving the reproduction and health of model animals."
#toxicbileapocalypse
-
So do you think there are any cases where restriction could be helpful?
I’ve read your article on daily excretion rates and it seems you said hepatic stores of 30ug/g is what the body wants as after that point it tends to dramatically increase the disposal of retinol.
Do you think restriction for a short while could be useful followed by introduction of retinol back into the diet with other things that may prop up the metabolism to help utilise it. It seems a lot of these low A people can’t go too long on it and end up resorting to eggs. I personally tried Low A for about a month now and each time I restrict to much I feel what I can only describe as though I am becoming dumber, I lose inspiration for life and just drift. Then as soon as I eat some cheese and or eggs I feel my gusto coming back again…
Is restoring thyroid function the best way to deal with this and some sort of mild restriction?
However going low A brought some relief in terms of anxiety and other problems like that but if I go to long I feel mentally impaired.
-
@Jakeandpace said in Conditional problems with vitamin A: a place for sane discussions:
So do you think there are any cases where restriction could be helpful?
I’ve read your article on daily excretion rates and it seems you said hepatic stores of 30ug/g is what the body wants as after that point it tends to dramatically increase the disposal of retinol.
Do you think restriction for a short while could be useful followed by introduction of retinol back into the diet with other things that may prop up the metabolism to help utilise it. It seems a lot of these low A people can’t go too long on it and end up resorting to eggs. I personally tried Low A for about a month now and each time I restrict to much I feel what I can only describe as though I am becoming dumber, I lose inspiration for life and just drift. Then as soon as I eat some cheese and or eggs I feel my gusto coming back again…
Is restoring thyroid function the best way to deal with this and some sort of mild restriction?
However going low A brought some relief in terms of anxiety and other problems like that but if I go to long I feel mentally impaired.
Just to clarify, the expert here is Kvothe. It's why I tried to get him to embark on a project for mentorship.
Yes, moderating any "nutrient" makes sense if it's doing more harm than good, but calls for alternative means to increase the tolerance to normal instead of finding comfort in labeling it as a toxin, as the poison A crowd do.
I don't know what you consider a short period, but to get to the therapeutic range, people need to be extreme and consistent. A month of restriction won't get you any lasting result and it's preferable to skip it.
If the issue is immunological, focusing on adequate metabolic rate (and the nourishment needed to sustain it) probably won't be enough. Compromised barrier integrity and disturbed gut composition can be the underlying problems.
Shared on the Garrey Pith Forum, but worth reposting here:
"Previous studies have demonstrated that serum retinol is the main determinant of VA disposal rate in rats with low to moderate VA intake (16), whereas VA status affected disposal rate in rats with higher liver stores (15). Our results appear to support those observed in rats with high liver VA stores (15) by showing that the model-predicted VA disposal rate was strongly correlated to VA total traced mass in Chinese (Fig. 3 A), U.S. (Fig. 3 B), and all subjects (Fig. 4 A). Moreover, when we compared VA disposal rate to serum retinol concentrations in all subjects, we observed that retinol concentrations were correlated with VA disposal rate (Fig. 4 B, C), indicating that serum retinol also contributes to whole-body VA disposal as previously reported (16)."
"[..]differences in VA nutriture will lead to changes in VA kinetics that will alter VA disposal rate to either conserve VA (VA deficiency) or prevent excessive accumulation of VA (VA sufficiency) even when VA levels are adequate."
-
@Amazoniac Thanks for your response with helpful citations. I think your distinction between vit-A "overload" vs. vit-A "toxicity" symptoms is important (i.e., neither implies the other): "The person doesn't have to be overloaded with poison A in the body to experience toxicity problems, these can happen at low intakes when the metabolism of a substance is deranged or if its addition influences pathways that are maladjusted." Agreed.
Your advice (to the post above) is another strong point for those of us who might have considered vit-A restriction is similarly well taken, namely, that vit-A restriction would have to be very strict and consistent (e.g., for multiple months, I'm supposing) in order to notice any meaningful effects.
Despite me being a likely candidate for carrying unusually high levels of vit-A in various concentrations across various tissues, I'll continue eating eggs, milk, cheese, pumpkin etc. in the absence of any discernable symptoms.
-
I believe it may be an estrogen problem for most of these people. All the papers by Mawson I've read seem to point towards an increase in retinoic acid at the particular diseased site, or a dis-regulation of retinoid signalling like in glioblastoma.
From this Ray article it seems estrogen is responsible for triggering certain inflammatory immune response like the chitinase enzymes etc. I wouldn't be surprised if it did the same with retinoic acid needlessly at the site of inflammation.
I think a lot of their benefits are as you say blunting the immune response but also I'd add a reduced endotoxin load. They all seem to do bad ("detox reactions") without any binders.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login