Everything about high blood pressure
-
From what I’ve read and experienced, it seems likely that cortisol is the main mineralocorticoid receptor ligand. So, if you have any chronic inflammation in your body(gut or otherwise), it is likely you will be unable to lower blood pressure until this is resolved. If that is the case, that should be the main focus.
-
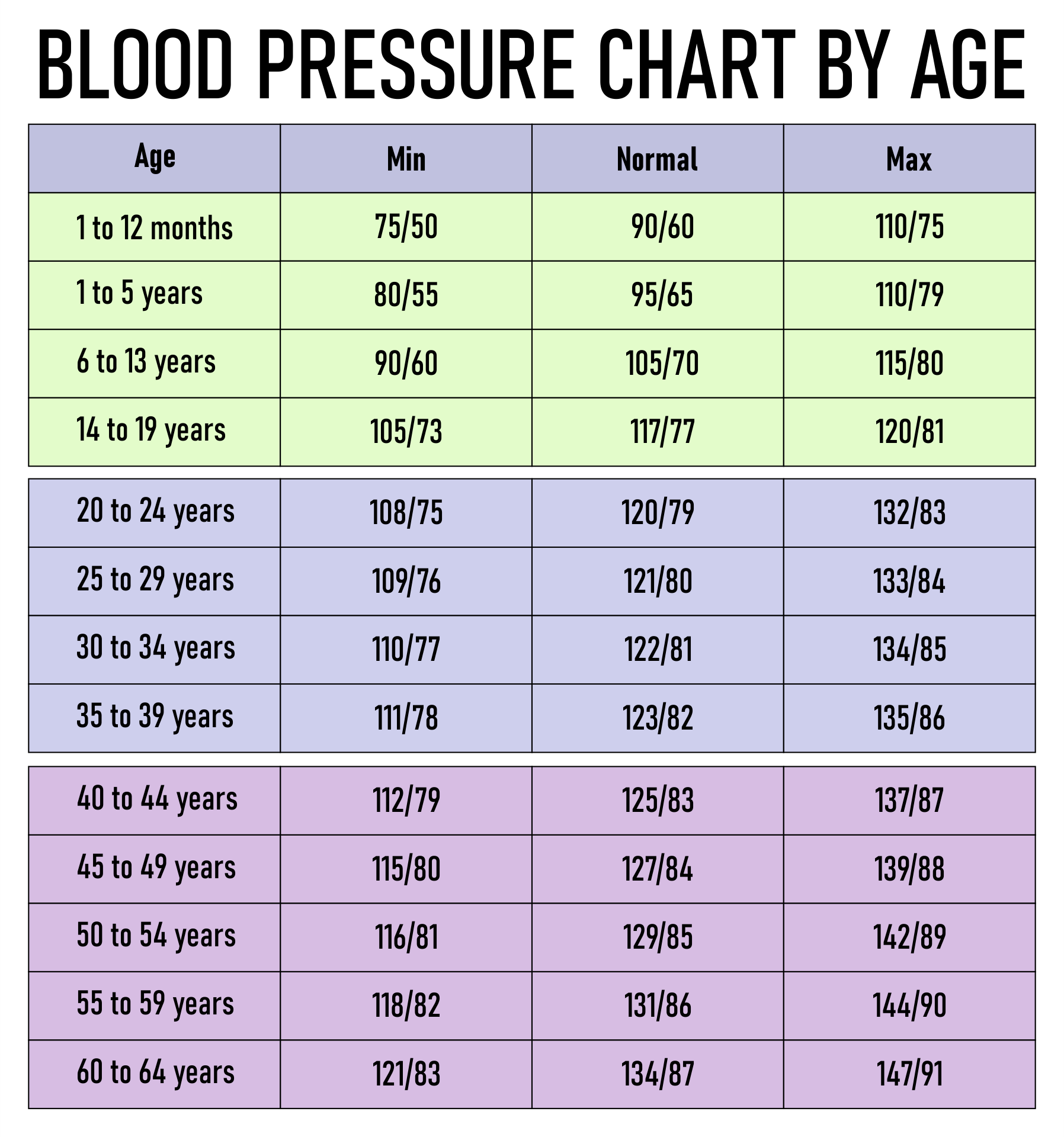
blood pressure should depend upon age. As we age, our vessels get less flexible and more clogged and we require higher pressure to prevent tissue hypoxia. People who are in their 60s or 70s or 80s are better off with 145/85 to 165/90 which is shown to be the best for longevity and healthy.
-
@Ecstatic_Hamster - I agree and your point is is a very important reminder. One size (120/80) does not fit all.
My GP retired and his replacement wanted to place me on a low dose blood pressure medication. My blood pressure measured in his office was 123/78. He told me that there were new guidelines and that both of my numbers were too high! There was no counseling about diet, exercise or weight. I declined his offer for medication. I supsect that he wanted to hand me a script for a 3 month supply and then have me return to his office every 3 months for the rest of my life to have my blood pressure checked and then write a new script. This is the medical treadmill. They treat the numbers but not the patient.
-
@Mulloch94 You are right salt restriction is not necessarily helpful for lowering BP. My question was specific to the situation Peat was talking about when estrogen is high. When he said ‘at first sodium falls’ made me wonder if later on sodium becomes harmful because it is being retained. Anyway, I tend to get the minimum required to restrain aldosterone, which is around 2000mg of sodium (a teaspoon of salt). I do use progest E but it has since stopped making a difference. I have a feeling that Dr. Peat would say we were not getting enough salt.
@DavidPS you have good BP. I can’t believe anyone would want to medicate such low numbers
-
@Peatly Yeah probably so, according to Haidut's post about sodium on the old forum we're both consuming low amounts of sodium relative to what's promoted.
But I think as long as we consume just enough to maintain proper mineral balance we should probably be fine.
-
@Peatly It's possible we could also supplement with sodium bicarbonate when we can't tolerate anymore salt. Sodium bicarbonate doesn't have the same effects on BP as sodium chloride.
-
@DavidPS said in Everything about high blood pressure:
He told me that there were new guidelines and that both of my numbers were too high!
That's insane he tried to prescribe you meds. Even ten points higher at 133/88 BP is still acceptable without any chemical interventions. Probably not needed until you're at 140 or higher.
-
@Mulloch94 - I agree about it being insane. But if a doctor prescribes a drug in accordance with the guidelines, he/she is not accountable for any negative health consequences of the prescription. I am thinking about increasing the risk of silent strokes.
Basically, IMHO the body regulates its blood pressure based on its needs. If your blood pressure is presistently high, you need to change your lifestyle (diet, weight, exercise). If you rely on drugs to lower your BP, your systolic pressure may not always be high enough to pump the blood (against gravity) into the upper parts of the brain. The end result could be a slient stroke which damges the brain and accumulate with time. The long term result is to zombify your brain.
I lowered my systolic pressure by about 15 points by lowering the amount of fat in my diet. Dietary fats are known to sludge the blood for hours and necessitates a rise in BP to feed blood to the brain.
Dr. McDougall has a very short video produced by Roy Swank (1909–2008) showing blood sludge and reuleux formation in the blood after a high fat meal. In the second video., Dr. McDougall states that there are no healthy fats. Here on the forum PUFAs (including fish oil) have been recognized as not being healthy. From a blood flow perspective, I could not find any evidence that saturated fats are healthy.
-
@DavidPS I haven't been convinced by anyone that saturated fat is inherently healthy. Probably best to keep all fats on the lower side. Peat echoed this logic, despite the large pro-saturated fat trend on the old forum. In one of those herb doctor call-in shows someone asked Ray if it would be best to focus on saturated fat as a prmiary source of calories and he flat out said no.
His words exactly was something like "Get as much sugar or starch as possible, and keep fats to a minimum."
I always found that to be like a checkmate against the pro-saturated fat people. Which is important, because I get a feeling a lot of the former keto bros keep falling back into this logic that saturated fat is good, when it's really just benign in the best of scenarios. Probably not even benign though. It's likely harmful just in different ways from PUFA. The problem with PUFA is they accumulate and disrupt the electron transport chain cause ROS.
But there's some evidence to suggest saturated fat causes endoxemia in humans, which also causes systemic inflammation. In fact, the study posted showed SFA's were worse at this than PUFA's. There's also data that refutes some of this, like dairy fat and coconut fat being good for combating obesity. But the endotoxin thing should be most concerning in my opinion. And if we're going to keep things in a Peaty lens, Ray himself seem to believe sugar AND starch was better than saturated fat.
-
@Mulloch94 - I have never heard any stories about someone who had a fat deficiency. If a person eats adequate calories, lipogenesis
provides the needed fat (and oftentimes more). It is my understanding that it is 100% saturated.PeatBot is is my tool of choice for keeping things within a Peaty lens. I read the sources listed at the end of the output. I consider PeatBot to be a bibilography generator. Here for example, William Brown caught my eye in the response to my question. With the help of PeatBot I found the interview that his work was discussed (Ray Peat KMUD: 9-21-12 Calcium and Phosphate Metabolism Full Interview).
User: is a low-fat diet healthy?
Peatbot: The context provided offers insights into a specific case where a low-fat diet, particularly one high in sugar and milk, had positive effects on an individual named William Brown. Brown's diet, which was essentially high in carbohydrates and calcium with a good calcium to phosphorus ratio, led to improvements in his health markers such as cholesterol levels, blood pressure, weight, and the cessation of migraine headaches. It also seemed to increase his metabolic rate and reduce feelings of fatigue.
However, it's important to note that the health effects of a low-fat diet can vary greatly from person to person. The context suggests that for some individuals, especially those with a PUFA (polyunsaturated fatty acids) overload, a diet high in carbohydrates and low in fat might be beneficial. It also mentions that the fats we synthesize from sugars are saturated and are not likely to be stored as excess fat because they don't suppress metabolism like polyunsaturated fats do.
The context also touches on the importance of having some fat in the diet for its effects on the intestine and nutrient absorption, and it suggests that if the fats are mostly saturated (as in butter, coconut oil, or beef or lamb fat), roughly a third of the calories from fat might be appropriate, though this can depend on individual factors like specific foods and activity levels.
Dr. Peat, whose views are represented in the context, seems to advocate for a diet that minimizes polyunsaturated fatty acids due to their breakdown into toxic fragments and inflammatory compounds. He also emphasizes the importance of sugars and minerals in fruits and milk for metabolic activation and prevention of free-radical damage.
In summary, while the context provides an example of a low-fat diet being beneficial for one individual, it also suggests that dietary needs can be highly individualized. It's important to consider personal health conditions, metabolic rates, and nutritional requirements when determining whether a low-fat diet is healthy for someone. Consulting with healthcare professionals and nutritionists is always recommended when making significant dietary changes.
-
From the real Ray Peat
“For about 40 years, the agriculture department was listing lard as a saturated fat. So there are hundreds of publications on so-called saturated fat damage, and they were using lard as their saturated fat. Two or three years ago, it came out, someone measured lard saturation and found that it was about 30% PUFA.” Ray Peat
"The things that are high in phosphate have some of the overlapping effects with the inflammatory things. Calcium, if you have a high ratio of calcium to phosphate, calcium happens to suppress the fermentation of fiber and starch in the intestine. So high calcium intake will actually reduce the production of the endotoxin as well as reducing the consequences of your reaction to the endotoxin. The saturated fats, having some fat in your food does various things that can be helpful. There's a germicidal effect of the fatty acids that helps to keep the intestine sterile and you should be able to absorb your fat by roughly half to two-thirds of the way down your small intestine where it's still sterile. But if you eat fat with a fiber, the fat helps to suppress the bacteria and it can help the fiber persist and go all the way through your intestine. So it can turn what would be a harmful fiber-supporting endotoxin into a useful sort of a bowel-stimulating bulk former.” Ray Peat
“Again, in the 1970s, I was attracted to it by reading an article in which they had fed several groups, I think it was 15 groups of rats on different diets, including either a high-fat, saturated fat, a low-saturated fat diet, a very high polyunsaturated fat diet, and a very low-fat diet with only polyunsaturated, and so on, so that they had 15 different compositions, very high-fat, very low-fat, pure saturated, pure unsaturated. And at the end of their life, the leanest rats were the ones that ate the saturated coconut oil diet, regardless of whether it was high-fat or low-fat. And the fat animals were the ones that had the pure polyunsaturated fat. Again, even a low-fat diet, if it was purely polyunsaturated, made them the fattest animals. So it wasn't the quantity, it was the unsaturation. In the last several years, people have started talking about the saturation index, meaning the proportion of saturated fats to polyunsaturated in your tissues, and cancer patients are very low on the saturation index. So it's not only obesity-producing, it's associated with high incidence of cancer to have highly polyunsaturated fat diet.” Ray Peat
-
-
@DavidPS I have to admit peatbot is not too bad but you can’t beat the real thing!
-
looks like I had the right hunch
the woman's PTH is double the reference range
high tCO2 in blood, high SB, ionised calcium in the upper range, normal vitamin D
-
@ursidae Good call. Please keep us posted. Would love to know how she resolves this.
-
This post is deleted! -
@DavidPS Yes indeed, a fat deficiency seems almost impossible unless you're eating some laboratory diet with isolated amino acids. There's really never a need a prioritize fat when we can prevent deficiency by just eating food. I think Walt Kempner's rice experiment pretty much vindicated this idea. His patients were eating only like 3-5% of their calories from fat and their health conditions only got better.
-
Calcium and riboflavin are two chemicals known to reduce blood pressure, given salt intake is sufficient.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login