Glucose loading cures everything?
-
But there's some sort of concert going on.
@ThinPicking said in Are Polls a Good Idea?:
Is it actually possible to substitute in either direction. Maybe just a temporary lack of control and engagement in some. Many ways a person can delude themselves. Misappropriate their condition and capability.
I don't know. So this isn't an objection. I'll be creating some posts on the subject at some point.
https://www.mdpi.com/1424-8220/22/23/9115
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7075501/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10002343/
https://www.ahajournals.org/doi/10.1161/STROKEAHA.123.040499
https://www.sciencedirect.com/science/article/abs/pii/S0306987719307145
https://www.sciencedirect.com/science/article/pii/S1568163721002865
https://www.frontiersin.org/articles/10.3389/fpsyg.2014.00278/full -
If glucose loading works, it hasn't been properly explained why it works.
When tissues cannot absorb and metabolize glucose, why does glucose loading work nonetheless. Perhaps it's because when blood glucose gets high, it triggers the polyol pathway, where glucose is converted to fructose. Unlike glucose, fructose is more easily absorbed and metabolized by tissues.
The question would arise "Why not simply take fructose? The answer is that fructose feeds gut microbes more readily and this can cause some gut problems.
Still, Stephens only focuses on glucose loading as a simple answer to brain lacking the energy to power itself. At least that is the impression I get, and I did not finish watching the video because I felt it is a waste of time. I felt he owes it to his audience explaining the role of having enough tissue oxygenation to fully use glucose to produce energy. Has he done this? He may know this, but he rather prefers to make his case for glucose loading by oversimplifying the case for glucose loading. He must look down on the mental capacity of his audience. Or he may just be practical, seeing his audience as cretins due to the brain already made inutile by lack of glucose.
-
This post is deleted! -
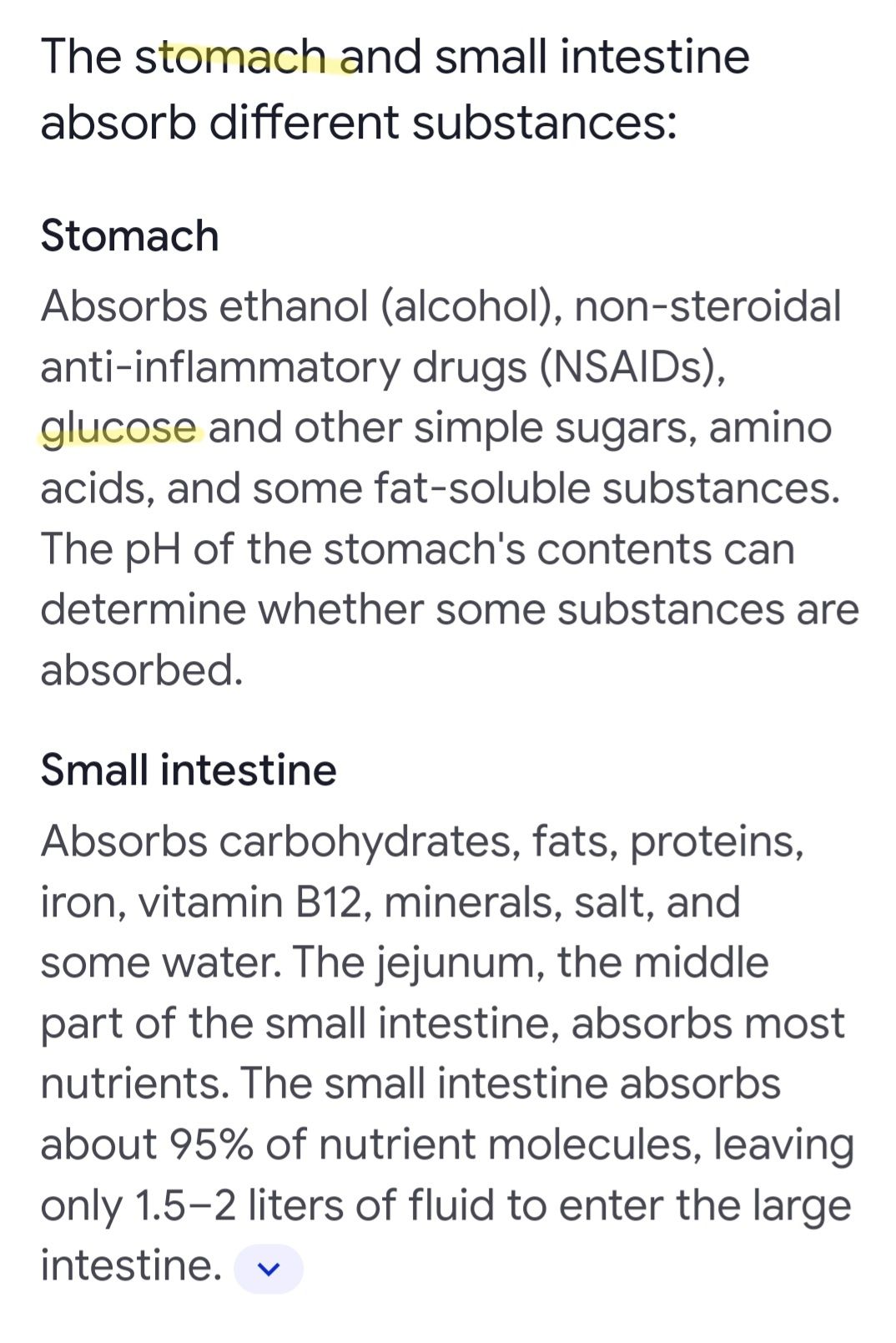
@yerrag I don’t have a definitive answer, but in his lectures he suggests that the glucose is digested in the small intestine, (prior to reaching potential issue with microbes in the large intestine-not sure where SIBO would come into play there).
He also mentioned in a lecture that in order to better understand why it works he would need volunteers for spinal taps and one other procedure, (I forget) that obviously no one is volunteering for. I personally wonder if using a radioactive substance in mice would lend any clarity on the how or why?
Personally I’m “lucky” to have suffered with poor dental health for years, and as such as soon as glucose goes in my mouth, my teeth get harder, whiter, and shiny/smooth. I’m not sure if this suggests that uptake or “digestion” is even taking place in the mouth, prior to the small intestine, but it’s what I’m experiencing, so I thought I’d throw it out there.
-
I don't know. I've been dextrosed 300g day for 4 days and it changed me. I sleep well, I don't get sugar crashes anymore but man kills my appetite. I eat way less and I don't lose weight, maybe it's water weight from insulin spikes?
-
@evan-hinkle said in Glucose loading cures everything?:
In the video, Smith says, maybe temporarily glucose could have a positive effect, (like filling glycogen stores) but long term any sugar powder is going to be bad. It seems to me, that this is exactly what Dr Stephens is suggesting… indicating that perhaps Smith has not looked too deeply into it.
What difficulty did you have with sugar that led you to dextrose Evan?
-
@yerrag said in Glucose loading cures everything?:
When tissues cannot absorb and metabolize glucose, why does glucose loading work nonetheless. Perhaps it's because when blood glucose gets high, it triggers the polyol pathway, where glucose is converted to fructose. Unlike glucose, fructose is more easily absorbed and metabolized by tissues.
Evan also mentions hydration of his eyes and better sleep some way up. Along with the teeth thing. My best bet remains that it's resolving a kind of edema. Drawing in structure, raising metabolism, which also produces structured water inherently. I would say filling in edema with structural components, but he also reported some welcome weight loss.
I just wonder at what cost. If this isn't created by or refined from nature. Why not the fructose. Or why would there be a preference for this.
-
@yerrag said in Glucose loading cures everything?:
Still, Stephens only focuses on glucose loading as a simple answer to brain lacking the energy to power itself. At least that is the impression I get, and I did not finish watching the video because I felt it is a waste of time. I felt he owes it to his audience explaining the role of having enough tissue oxygenation to fully use glucose to produce energy. Has he done this? He may know this, but he rather prefers to make his case for glucose loading by oversimplifying the case for glucose loading. He must look down on the mental capacity of his audience. Or he may just be practical, seeing his audience as cretins due to the brain already made inutile by lack of glucose.
Also I had the same difficulty continuing his interview with Torrens. Had to persevere.
-
@ThinPicking I never had positive results from fruit. I had painful oral health, (teeth and gums) symptoms of liver issues, (need to eat frequently-poor glycogen stores, mood swings, waking at 2am) weight gain. I don’t know why, I’ve been “Peating” for almost 6 years now, but fruit just doesn’t provide the relief or satisfaction of dextrose.
Also, anecdotally, my sister-in-law stopped a migraine at the point of halo with a single glucose tablet just yesterday! She has never in her life stopped a migraine once the halo came.
I just don’t know what to say guys… it works?
-
@Androsclerozat said in Glucose loading cures everything?:
I don't know. I've been dextrosed 300g day for 4 days and it changed me. I sleep well, I don't get sugar crashes anymore but man kills my appetite. I eat way less and I don't lose weight, maybe it's water weight from insulin spikes?
Try this. Maybe. Eat normally for breakfast and lunch, salt those meals more heavily than you're used to. Reserve the dextrose load for later in the day.
Or any other way to get your salt load up prior to consuming it. If you were to restrict whatever other carbs you'd normally eat, and increase your salt. You'd probably start craving those carbs ravenously anyway. I might describe the interim as a structural derangement. Subsequent craving a hormonal response to drive you.
@Androsclerozat said in Glucose loading cures everything?:
I eat way less and I don't lose weight, maybe it's water weight from insulin spikes?
Another indicator for fluid dynamics. At least. We'll figure this out.
Dextrose is commonly administered with saline IV under certain conditions. Maybe I'll jump there. Why didn't they design those protocols with something more in line with nature.
-
@evan-hinkle said in Glucose loading cures everything?:
I just don’t know what to say guys… it works?
This. 100%. For your health and wellbeing.
I appreciate you describing that other stuff to no end.
-
@evan-hinkle Apologies if you already said...how much are you taking?
-
I'm not sure if it does not have any negative tradeoffs. In going to the polyol pathway, if the sorbitol produced from glucose does not convert to fructose entirely, the sorbitol could cause osmotic stress within the eye and lead to diabetic retinopathy.
But this is just a lazy search using Google, which I have to take with a grain of salt.
-
@S-Holmes I’m taking 60g 4 times a day
-
@evan-hinkle said in Glucose loading cures everything?:
@yerrag I don’t have a definitive answer, but in his lectures he suggests that the glucose is digested in the small intestine, (prior to reaching potential issue with microbes in the large intestine-not sure where SIBO would come into play there).
This is true with glucose. Which is why it's better to take glucose than fructose as there will be some sugar that gets into the large intestine, and glucose is much less likely than fructose to feed the gut microbes in a way that causes gut issues.
He also mentioned in a lecture that in order to better understand why it works he would need volunteers for spinal taps and one other procedure, (I forget) that obviously no one is volunteering for. I personally wonder if using a radioactive substance in mice would lend any clarity on the how or why?
I think it's a given the brain uses sugar for energy almost exclusively, so glucose loading would benefit the brain, but not simply because glucose van be delivered to the brain, but because the brain cells can use the glucose to produce the energy needed by the brain. But how efficiently it produces energy is dependent on factors such as how well oxygenated the brain tissues are as well as how freely blood is perfused through the capillaries, which is dependent on the health of the microcirculation.
I don't know much about spinal taps and what the fluid it draws consist of, to know how it would help find answers.
Personally I’m “lucky” to have suffered with poor dental health for years, and as such as soon as glucose goes in my mouth, my teeth get harder, whiter, and shiny/smooth. I’m not sure if this suggests that uptake or “digestion” is even taking place in the mouth, prior to the small intestine, but it’s what I’m experiencing, so I thought I’d throw it out there.
Interesting. I'm sure your dentist is just as flummoxed. I am just as intrigued.
-
@evan-hinkle Do you know of any reason why one or two doses a day couldn't be used to sweeten my coffee? I've been doing that but not sure if it's helpful. I am also somewhat concerned about gaining weight.
-
@S-Holmes I’ve heard some people suggest that coffee could be somewhat contrary to the glucose therapy. However those people don’t tend to share a bioenergetic framework through which they look at life.
Me personally, my first “dose” of 60g is “split” amongst 8oz of juice, and two 8oz cups of coffee with milk. My three remaining doses are typically just sprinkled on a meal, or in a smoothie. But I start my day with 8oz of juice with 1/4 tsp baking soda and 20g of dextrose, (I mix the dextrose with the juice first, and then react the baking soda). Then right after I drink my 2 coffees, 8oz coffee, 4oz milk, 20g dextrose, (times 2).
-
@evan-hinkle Excellent! I was hoping to use it more in place of sucrose and it sounds like you're doing that as well, and with positive results!
-
@S-Holmes said in Glucose loading cures everything?:
@S-Holmes It makes sense to me. If your brain is well fed, it can stop signalling the body to release/make more fuel, which can't get into the brain anyhow (due to stress and injuries). So the glucose stops the cascade by nourishing the brain, bypassing the digestive process and going directly to the brain where it's needed.
How is the digestive process bypassed? I fail to see the logic. One way the digestive process is bypassed is by IV feeding. But I don't know if this is what you mean.
-
@yerrag This is the best I can do for now.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login