Bile can serve as a reservoir for funghi, making them harder to treat
-
Glad that it worked for you the 2nd time around. It could be about cycling, as that is something I forget to do at times. It it could be that you changed that made your interior more conducive to being fixed.
-
@dapose You hit many right notes there. Usually there is an imbalance and that leads to a dominance that is seen as pathogenic. Perhaps we should see restoring balance as the goal. We never really kill or eliminate like genocides are natural, we only discourage dominance because uneven playing fields make it happen. Intentional or nor.
Temporal thinking is the faculty that’s
engaged by an enriched environment, but it’s
wrong to call it “thinking,” because it’s simply
the way organisms exist... - Ray Peat Nov 2017 Newsletter -
@Mauritio said:
we need small and hydrophilic molecules for an anti-fungal effectIm looking for anti-fungal candidates that fit the above category:
Encapsulated calciumhypochlorite granules ("Chloryte") may fit this bill for the upper GI and various deep tissues. It's rather rough and destructive and not a thing to do for more than two weeks at the very most, IMO.
@Mauritio said:
I took Haarlem oil daily for a while.
I believe it contains turpentine and sulfur. I got less and less of an effect as time went on so I stopped. But I recently reintroduced it and found that cycling it, seems to maintain its effects.Turpentine (or more generally monoterpenes) reduce hepatic cholesterol synthesis, thereby reducing the cholesterol-saturation of bile which is then able to gradually dissolve cholesterol "plaque" or even proper stones along the bile ducts and in the gall bladder. That improves the biliary milieu along with better biliary flow. It's a very long-term process, however. It takes several months of taking monoterpenes ("Rawachol" capsules or tincture is an OTC product) 2-3 times daily. Tudca or Udca works well together with monoterpenes.
@Mauritio said:
I'm not sure how the treatment should look.
Increasing transit speed and frequently emptying the gallbladder by eating fiber, using specific supplements like FXR-agonistsTudca and Udca also reduce the same enzyme of hepatic cholesterol synthesis, while additionally altering the bile acids composition towards being much more hydrophilic and less sticky, and also increasing the bile salt export pump for an in overall much greater bile flow (less stasis).
I'd rather use those daily instead of doing any more gall bladder flushes ever again (which only work in a very mechanical and macroscopic way). -
@yerrag
Well said Ye!
I would say heavy hitters in the militaristic approach to a balanced system would be Castor Oil packs on the skin over the liver.
Higher dose Aloe Vera Juice.
Oregano oil + activated charcoal.
Russian Sauna. Or fever.
And Swedish Bitters one shot in warm chamomile tea.
The big guns!
Have you ever tried clove tea for your lungs!!?? Supposed to be great!!! -
@Sunniva said in Bile can serve as a reservoir for funghi, making them harder to treat:
(DMSO) inhibits the germination of Candida albicans
That is so interesting . You just helped me to connect the dots.
Several times when I used Melanon topically on the area above my liver/gallbladder I experienced fungal die off. I attributed it to apigenin or naringenin, but it might as well be the DMSO.
Apigenin and naringenib are also anti-fungal. They're also small molecules, but not hydrophilic. But still Melanon should be a very effective anti fungal applied topically.
https://pubmed.ncbi.nlm.nih.gov/29346565/
https://pubmed.ncbi.nlm.nih.gov/33934490/If the gallbladder is so hard to reach for anti-fungals maybe topical is the way to go.
Maybe using some anti-fungal IdeaLabs supplements over the gallbladder would be good, ideally one that uses DMSO as a solvent.Alternatively dissolving MSM in DMSO should help. It is a small, hydrophobic molecule and it dissolves in MSM so it might be very potent if delivered directly to the gallbladder via topical application.
-
@Mauritio
Very nasty! Thanks for pointing me back to this thread.
One thing I was immediately wondering about is whether the less-lipophilic fluconazole would then be more potent against bile fungi than the significantly more lipophilic itraconazole, even though fluco is quite completely being excreted renally and itra biliary.
But the answer lay in your linked study: Fluco was shown to be useless in bile. Utterly.
There no mentioning of itra in this context. Only a remark, that fungi increase their itraconazole-resistance in the presence of cholesterol. However, this mechanisms affects all azoles. Essentially, candida and other fungi can salvage exogenous cholesterol to make up for loss of ergosterol synthesis and are thus less affected by the inhibiting impact of azoles.So how to tackle these biliarly persisters?
I doubt they will only serve as a reservoir without already being harmful where they are. In your linked studies it says, C. albicans hyphenates upon contact with bile acids. I therefore assume they do bad things already in the liver and gallbladder and potentially alter the function of these organs or of the bile composition. @bearwithmeThe water-soluble flucytosine is available as 500mg tablets (ANCOTIL) on prescription for specific systemic fungal infections... certainly nothing anyone would easily obtain officially from a doctor because of a hunch of biliary fungal persistence!
I had never heard of it before.
Side effects are kind of the usual; don't get pregnant or impregnate anyone else within 6 months, blood cell discorders, skin detachment, fatal hepatic lesions, hypokalemia and heart troubles, the whole cluster of confusion, headaches, vertigo, neuropathies, hallucinations as well as respiratory impairments or arrest and reduced kidney functions.
What do you peeps reckon - is it wortwhile to try out?@Mauritio said in Bile can serve as a reservoir for funghi, making them harder to treat:
Im looking for anti-fungal candidates that fit the above category:
MSM Small molecule and highly water soluble , fits the bill.Any info on how methylsulfonylmethane would be antifungal?
Oregano oil or winter savory oil mostly for the carvacrol and thymol are again strongly lipophilic.
Berberine is strongly synergistic with azoles and can overcome azole-resistance.
Propolis extract is antifungal as well and can overcome azole-resistance.
Boron.
Balsamic turpentine may be mostly anti-biofilm.
Especially boron may be mostly preventative at regular low doses but tbh I'm really disappointed with all of these on their own not being anywhere near to being effective on their own.Maybe a topical antifungal like nystatin or amphotericin B for the GI lumen over quite a long term, plus a combination of systemic substances: boron, berberine, propolis extract, + pharmaceutical antifungal?
-
@Mauritio said in Boron supplements:
@CrumblingCookie I agree with you on subclinical fungal infections.
They're very hard to get rid of. I posted a study about fungi hiding in the gallbladder when attacked. Let that sink in.It's just as bad when we look into CNS persistence of fungal infections in chronic brain disorders, Alzheimers and dementia:
Tulane University & Tulane National primate research center, 2022

The potential contribution of pathogenic microbes to dementia-inducing disease is a subject of considerable importance. Alzheimer’s disease (AD) is a neurocognitive disease that slowly destroys brain function, leading to cognitive decline and behavioral and psychiatric disorders. The histopathology of AD is associated with neuronal loss and progressive synaptic dysfunction, accompanied by the deposition of amyloid-β (Aβ) peptide in the form of parenchymal plaques and abnormal aggregated tau protein in the form of neurofibrillary tangles.
Observational, epidemiological, experimental, and pathological studies have generated evidence for the complexity and possible polymicrobial causality in dementia-inducing diseases. The AD pathogen hypothesis states that pathogens and microbes act as triggers, interacting with genetic factors to initiate the accumulation of Aβ, hyperphosphorylated tau protein (p-tau), and inflammation in the brain. Evidence indicates that Borrelia sp., HSV-1, VZV (HHV-2), HHV-6/7, oral pathogens, Chlamydophila pneumoniae, and Candida albicans can infect the central nervous system (CNS), evade the immune system, and consequently prevail in the AD brain. Researchers have made significant progress in understanding the multifactorial and overlapping factors that are thought to take part in the etiopathogenesis of dementia; however , the cause of AD remains unclear .
“It has been suggested that Aβ functions as an antimicrobial peptide. Interestingly, C. albicans was found to be sensitive to synthetic Aβ and brain homogenates from AD patients that were capable of inhibiting fungal growth [178]. Additionally, it was demonstrated that Aβ protects against C. albicans in glial cells as well as invivo in nematodes [179]. ”
“Alonso and colleagues provided extensive evidence that disseminated mycoses are potential causative agents or risk factors for AD [173,180]. Different fungal genera detected in AD brain tissue include Malassezia, Fusarium, Candida, Cladosporium, Alternaria, and Botrytis [181]. An analysis of CSF revealed significant levels of Candida albicans and Candida glabrata in samples from AD patients. Approximately >89.6% of serum from AD patients tested positive for antibodies to Candida compared to 8.8% for controls [173].”
“The different species that were detected included Saccharomyces cerevisiae, Malassezia globosa, Malassezia restricta, and Penicillium. Furthermore, this group detected yeast and fungal proteins, including (1,3)-β-glucan, fungal polysaccharides, and mycoses, in the peripheral blood of AD patients, which suggests that a chronic fungal infection may increase the risk of dementia [173,180]. More strikingly, yeast-like cells and hyphal structures were observed in CNS tissue from AD patients using polyclonal antibodies against a variety of fungi [181].
Pisa et al. also provided strong evidence for fungal infection in AD patients [170]. Brain sections derived from AD patients showed that all were infected with fungi [170]. Fungal material was detected intra- and extracellularly in the neurons of tissues of AD patients, but no fungal material was observed in tissue from control individuals [170]. Moreover , fungal DNA and proteins were also found in brain regions including the frontal cortex, hippocampus, cerebellar hemisphere, and choroid plexus but not in control patient tissue. ”
-
idk about in context of bile, but iron chelation in fungi via doxycycline makes fluconazole anti fungal against some candida rather than just fungistatic or no effect. aspirin is also an iron chelator.
there’s a study that suggests organ cancers often come with fungal infection of that organ too.
fwiw the warnings about ketoconazole being particularly liver toxic are apparently not actually proven. the symptomatic liver damage incidence rate in all the azoles is about the same.
overall for fungal issues i think the patient gets treatment with a normal pharmaceutical antifungal dose and length (could be months), and then keep the antifungals on hand to pulse dose as needed if symptoms return. and then use things like aspirin and doxycycine, include some niacinamide, sunbathing and nutrition etc to keep the stuff in check. total eradication of fungi seems impossible on a realistic sense
if bile is a reservoir for fungi maybe just eating high bile binding foods regularly can flush it out. rather than recirculating bile more
-
@CrumblingCookie nystatin is pretty weak ime but i guess it depends on which fungi
ketoconazole cream works way better ime but idk what strains it is working agaisnt. i think mallesseziaberberine seems interesting, is it peaty ? it isnt right, because it is like metformin and metformin isnt peaty
-
Thanks for sharing.
Indeed I currently find myself in a situation wherein I don't know for how long in total to continue fluconazole. Months? It costs about $60/week for me. And it's difficult to say which depressive mental effects are true sides and which are due to various degrees of die-off.
I wonder what role the continous re-infection from bile plays in commonly required treatment length. The notion of it being impossible to clear from tissues is what I find unsettling, too.
Have started to add in berberine today, 500mg thrice daily. Along with ample propolis extract twice daily.
Luckily I've failed to make it to the store in time and stumbled upon some garlic in my kitchen drawers and have read up on allicin again.
One half to a full garlic bulb per day is allegedly a good guideline for powerful effects (about 1mg allicin per kg BW from 3-5mg allicin per g fresh garlic). Ground it/crush it, let it rest for 10 minutes for the allicidase to do its work before diluting it in food or adding any acids like vinegar.@sunsunsun said in Bile can serve as a reservoir for funghi, making them harder to treat:
iron chelation in fungi via doxycycline makes fluconazole anti fungal against some candida rather than just fungistatic or no effect
That study is in-vitro and super misleading however, because few antibitiocs, if any other at all, are as fungal-infection promoting as the tetracyclines because of their powerful, continuous inhibition of phagocytosis lasting for days even after stopping further intake. Tetracyclines are one of the main risk factors for fungal infections in literature. Ime they are very overhyped and terrible.
As for ketoconazole I'm wary of its unique VDR antagonism which essentially inhibits innate immunity and reduces xenoautophagy of intracellular endomyceles. That also essentially makes ketoconazole topical creams a powerful antiinflammatory for skin conditions, saving the extra prednisolone so enamored by dermatologists.
-
-
@sunsunsun Wax moths? They don't even have neutrophils and I won't deep-dive into finding out how their hemolymphs specifically compare to human or mammalian neutrophils.
I really do harbor strong apprehensions against the potential (mis)use of doxy on fungal infections.What I would much rather do is oral terbinafin + fluconazole.
The terbinafin by itself is useless against many fungi species but by disturbing an earlier point (Erg1) in the sterol biosynthesis pathway it is synergistic with azoles (which act upon Erg11).
allegedly it strongly inhibits expression of the fungal efflux pumps responsible for azole resistance!
(! Berberine is the one which inhibits efflux pump expression. I had mixed it up).
This still won't tackle activitiy in the biliary tract, though.I've done some more reading of publications on biliary / gallbladder candida / fungi.
Fungi can be causes of calculous (lithiasic) or also acalculous cholecystitis with or without mixed bacterial infections (Escherichia coli, Enterococcus, Klebsiella, Enterobacter, Clostridia).
Even in such rare and often fatal cases that happened to be documented, candidemia was rare despite frequent (almost always) fungal infection of other organs.https://pubmed.ncbi.nlm.nih.gov/8862389/
https://pubmed.ncbi.nlm.nih.gov/28703118/
https://pmc.ncbi.nlm.nih.gov/articles/PMC8764969/
https://pmc.ncbi.nlm.nih.gov/articles/PMC12338181/
https://pubmed.ncbi.nlm.nih.gov/24474028/
https://pubmed.ncbi.nlm.nih.gov/8207288/I don't have visible gallbladder wall thickening or distention or an obviously, universally accepted liver disease (except for hepatomegaly) but if I had I sure as hell would want to insist on flucytosine, or flucytosine + i.v amphotericin B along with any broad-spectrum antibiotics and before mutilating surgeries they'd offer.
Have looked more into berberine again, too. It's impossible to achieve its antimicrobial concentrations (at least 0.1mg/mL) systemically. Serum concentrations are about 0.5 - 16 ng/mL. I.e. 0.000005 mg/mL. Ridiculous!
The berberine in practical doses of 500-1500mg will thus be acting mainly within the GI lumen in support of oral Ampho-B. Berberine has low absorption but some will spill over to reach the liver for extensive first-pass metabolism, yet probably not into biliary ducts. -
Great points, guys.
My current working hypothesis is rotating and combining several anti fungals daily + keeping bile flowing.
If i don't rotate the antifungals they seem to loose effect surprisingly quickly.
But what is obvious from many studies, is that combining certain anti fungals can drastically increase their effectiveness. Nystatin is synergistic with thymoquinone and also thymol IIRC.The other important part is to keep bile flowing and excreting it. The lowtoxin crowd actually has a point there. Inducing a bile dump seems very therapeutic to me and followed by certain time of remission/ relieve.
So having adequate fiber intake seems important. Pectin is helpful, vitamin D and K as well.
I also ordered an herb that's used for cholestasis in TCM called Artemisia capillaris it has a lot of studies on liver health and general anti-inflammatory effects. -
@sunsunsun said in Bile can serve as a reservoir for funghi, making them harder to treat:
idk about in context of bile, but iron chelation in fungi via doxycycline makes fluconazole anti fungal against some candida rather than just fungistatic or no effect. aspirin is also an iron chelator.
Makes sense. I've been using an iron cast pan for years and my ferritin came back very high.
Maybe that contributed to my susceptibility to (fungal) infections.@sunsunsun said in Bile can serve as a reservoir for funghi, making them harder to treat:
total eradication of fungi seems impossible on a realistic sense
if bile is a reservoir for fungi maybe just eating high bile binding foods regularly can flush it out. rather than recirculating bile more
Yes agreed


-
@CrumblingCookie said in Bile can serve as a reservoir for funghi, making them harder to treat:
Any info on how methylsulfonylmethane would be antifungal?
They say it's the sulfur in it. There's not a lot of evidence for that though. From my experience it is definitely anti-fungal.
I suspect it can chelate metals. Usually that doesn't just involve the bad heavy metals but also the good ones. So Id make sure to test my minerals and keep intake high when taking it long term. -
For what it's worth, let me throw in some tidbits from what I've conjectured over my 2 decades of trying to lower my blood pressure. I've done a lot from eliminating a lot of periodontal bacteria that has translocated to my vascularure to chelating lead lately using Emeramide. Through a process of elimination of these possible causes, I have been halfway successful only though in lowering my blood pressure. From 260/160 to a current 169/110, I still have ways to go.
But I still some light at the end of the tunnel though. And it is something I have overlooked. As fungal infection has always been under the radar and an afterthought inmedical circles. Doxtors would treat bacteria with antibiotics, and rarely talk about fungus. A confinement in a hospital would see a patient get well from antiiotic administration, but a discharge would be delayed only because the good doctor for some hunch decides to give some antifungals..
I would later realize that some antibiotics are known to transform bacteria into cell wall- deficient microbes that are harder to kill because they lack this cell wall which is used to kill microbes with antibiotics. This transformation from bacterial form to a form halfway between bacteria and a fungi ia at the hear of a ' competing medical dogma called terrain theory, which is opposed to the mainstream model based on herm theory- where all microbes are accepted as being static in nature, and do not pleomorph, as would be what happens when commensal and regulatory (aka friendly bacteria) turn from Dr. Jekyll into Dr. Hyde, and become pathogenic.
But this should explain to me why it has become common practice for doctors to administer antifungal drugs after successfully treating a patient with antibiotics. But they cannot explain why, for to say the real reason is to somehow agree that terrain theory is real, which is anathema to their cornerstone germ theory.
But back to my vexing problem of fixing my high BP problem, which is on its 26th year.
Lately, I had began taking artemisia annua tincture which saw me successfully lower my BP from 200./150 to 150/100. I took this as an antifungal to hyphal aspergillosis (aspergillus niger is also known as black mold. How I got this is another story).
It would be nice if my BP kept going down to 120/80. That would be a nice end to this story.
But my BP held at around 150/100 - 160/110. I was still urinating foamy urine. And I realize that this is the result of a continuing activation of neutrophils and macrophages th as t I would conclude from my CBC test, showing my wbc to be high and my neutrophils and monocytes to be high.
Even as my eosinophils have gone down as the large hyphal aspergillus fungal parasite colony have been markedly reduced. But the fungus took on a smaller form called a clamydophore. And in this form, more neutrophils and macrophages were needed to kill or neutralize them.
This is the reason why in my CBC test, there would be a high count both in neutrophils and monoxytes.Yet Iinflammation and oxidative stresses from ROS being produced and spilling over to destroy adjacent tissues would keep occurring, and that my body would have to use its antioxidants to protect tissues from.being destroyed. The main extracellular antioxidant would be called upon again, and albumin would be oxidized and excreted in urine. Which would explain foam in my urine. As well as mynhigh BP as my albumin stores in plasma would be insufficient to hold on to salt, with salt being needed to keep my plasma and blood volume high enough. The body compensates by increasing blood pressure.
But this fungal presence is hard to destroy. As you would concur. What I am trying now, in addition to turpentine and artemisia annua, is the use of Lugol's Iodine. In the next weeks and months, I will find out.
Looking back, I can't help but see why my LDH has always been high at around 260. I think it is because I have hemolysis. Under the radar. It is from an underlying fungal presence that needs to feed off iron from red blood cells it breaks down.
Since heme oxygenase enzyme breaks down the heme from hemolyzed red blood cells, the carbon monoxide could also explain why when I look at my heart rate chart, I would see occasional transient sharp drop in my heart rate even when my spO2 chart says I have a lot of oxygen at that given time. It is because a typical.oximeter cannot distinguish carbon monoxide from.oxygen, and the carbon monoxide is masking as oxygen, even as my heart cannot use the carbon monoxide to produce energy. I have a bit of carboxyhemoglobinemia. That is how I see it. And that would be a result if an ongoing case of chronic low level hemolysis caused by iron-hungry aspergillus fungi. The same fungi that is causing high BP stealthily.
Fungi remains as a. bogeyman to us.
-
@Mauritio taurine for bile excretion actually seems better than TUDCA at their relative normal doses (3g per day for taurine vs 500mg per day for TUDCA)
-
Result or (mutualistic) cause? It's pointing to the latter!
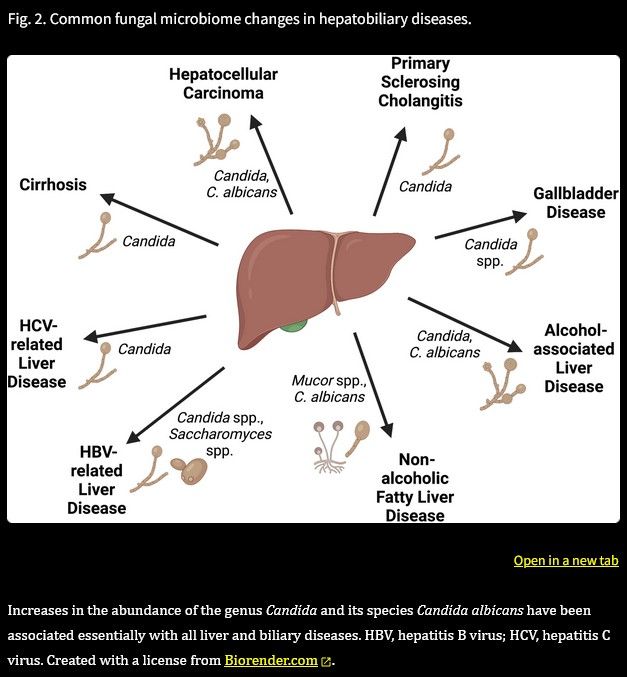
Fungal infections and the fungal microbiome in hepatobiliary disorders, 2022
@mauritio and others I urge you to read through the whole paper. It's a very scientifically sober and factual work which converges various interrelated aspects.
Excerpts (it appears almost necessary to quote the whole thing):
Although patients with cirrhosis already have elevated faecal levels of Candida [111], patients with HCC were found to have even higher faecal proportions of Candida and C. albicans than patients with cirrhosis, but lower proportions of the genera Kazachstania, Debaryomyces, Xeromyces, Amorphotheca, and Blastobotrys [122]. In a mouse model of HCC, gavage with C. albicans resulted in exacerbated HCC volume, which was dependent on the nucleotide-binding oligomerization domain-like receptor family pyrin domain-containing 6 (NLRP6) inflammasome [123]. Moreover, development of HCC in a patient with cirrhosis increases their risk of oesophageal candidiasis (OR 10.04) [113].
Specific serum anti-C. albicans IgG and IgM titres are increased in patients with AUD vs. controls, and interestingly, the anti-C. albicans IgG titre (but not the IgM titre) decreases significantly in patients after abstinence [55]. These changes parallel elevated faecal proportions of C. albicans in patients with AUD (vs. controls), which decrease after abstinence [55]. Similarly, plasma anti-C. albicans IgG titres are increased in patients with NAFLD and advanced fibrosis (F3-F4) vs. patients with NAFLD and no/early fibrosis (F0-F2) and vs. controls, and anti-C. albicans IgG titres correlate with the faecal C. albicans/S. cerevisiae log ratio [56]. Anti-C. albicans IgG titres hence correlate with disease activity in ALD [55] and NAFLD [56], indicating more systemic exposure to C. albicans in more severe liver disease.
Candidalysin is a secreted cytolytic peptide toxin from C. albicans that directly damages epithelial membranes, triggers a danger response signalling pathway and activates epithelial immunity [129]. C. albicans strains lacking this toxin do not activate or damage epithelial cells and are avirulent in animal models of mucosal infection [129]. The extent of cell elongation 1 (ECE1) gene encoding candidalysin was more frequently present in the stool of patients with AH than AUD [98]. Further, mice gavaged with wild-type ECE1-positive C. albicans had significantly higher serum alanine aminotransferase (ALT) levels, hepatic triglycerides and inflammation than mice gavaged with ECE1-negative C. albicans in a 2-week ethanol binge model, supporting the notion that ECE1-positive C. albicans exacerbates ethanol-induced steatohepatitis in mice [98].
Secretory IgA also binds ECE1-derived candidalysin, though this binding is reduced in patients with Crohn’s, indicating fungi-related immune dysregulation [130].
Antifungal treatment improves liver disease in various mouse models, including ethanol- and western diet-induced steatohepatitis [56, 97, 131]. Further, colonisation with C. albicans [98, 123] or Malassezia restricta [99] exacerbates liver disease. Therefore, fungi and their products contribute to liver disease.
Chronic alcohol administration increases mycobial populations and the translocation of fungal beta-glucan into the systemic circulation in mice [97, 131]. Oral administration of the antifungal amphotericin B reduces faecal fungal overgrowth and beta-glucan translocation [97]. Antifungal treatment with oral amphotericin B or caspofungin prevents ethanol-induced liver disease in mice without changing plasma bacterial lipopolysaccharide levels [97, 131].
Beta-glucan induces liver inflammation via CLEC7a on Kupffer cells, as shown in experiments employing bone marrow chimeric mice [97]. CLEC7a-dependent activation of caspase-1 via NLRP3 [134, 135] leads to increased inflammatory IL-1β expression and secretion, which subsequently contributes to hepatocyte damage and ethanol-induced liver disease [97]. CLEC7a also plays a role in diet-induced steatohepatitis, since its hepatic expression is significantly increased in patients with NASH and mice on a high-fat diet, whereas Clec7a-deficient mice and mice treated with a Clec7a-antagonist are protected from diet-induced steatohepatitis and fibrosis [136].
Rats infected with C. albicans by intraperitoneal injection develop hepatic steatosis, increased serum ALT levels, inflammatory markers, and pronounced lipid peroxidation [137]. This raises the question of how C. albicans causes liver disease. One effector could be its secreted cytolytic toxin candidalysin. Candidalysin exacerbates ethanol-induced liver disease and is associated with increased mortality in mice [98]. Candidalysin does this independently of Clec7a
Candidalysin can damage primary hepatocytes in a dose-dependent manner in vitro and is associated with liver disease severity and mortality in patients with AH [98]
The PGE2-producing fungus Meyerozyma guilliermondii was increased in mice with ethanol-induced steatohepatitis [131]. Further, supplementation with Meyerozyma guilliermondii worsens ethanol-induced liver disease
Concurrent administration of an antifungal also abrogates PGE2 formation and ethanol-induced liver disease [131].
Moreover, C. albicans is a potent inducer of the Th17 response via PGE2; PGE2 is induced by the C. albicans components mannan and β-glucan that are recognised by the mannose receptor and the Clec7a/Tlr2 pathway, respectively [147, 148].
C. albicans has evolved the capacity to produce PGE2 from arachidonic acid to promote its own colonisation in the host gut [152–154]. C. albicans mutants lacking PGE2 production (genetically missing ole2, a fatty acid desaturase) are unable to colonise the murine gastrointestinal tract
Key points:
Despite a relatively small number of fungal cells in the human body, fungi are involved in the development of liver and biliary diseases.
Various rodent models of fungal microbiome (mycobiome) modulation, including increasing the fungal burden (e.g. colonisation with fungi) or decreasing the fungal burden (i.e. via antifungals), have demonstrated the impact of the mycobiome on hepatobiliary conditions.
Fungal products including toxins and metabolites can exacerbate liver and biliary diseases.
In particular, the genus Candida and the species Candida albicans play a central role in the pathogenesis and progression of essentially all hepatobiliary conditions.
Serum antibodies against fungal populations have predictive value with regard to disease severity and survival in hepatobiliary diseases.
Conclusions
Mycobiome changes have now been established in essentially all hepatobiliary conditions. However, they are still a kind of dark matter, as we often do not know their true identity and characteristics, since we cannot culture many of them.
Further, they do not colonise mice easily, so we do not have good mouse models. Nevertheless, we know that some fungi are hepatotoxic themselves and not just bystanders – for example, rodents colonised with C. albicans develop liver disease without additional stimuli.
Fungi might hence possibly exacerbate liver disease in a two-hit model, one hit being alcohol, western diet, or a toxin, and another hit being the presence and deleterious impact of fungi.
We are learning more and more about the mechanisms by which fungi contribute to liver disease, be it via fungal cell wall components or secreted toxins, such as beta-glucans or candidalysin, or fungal metabolites including prostaglandins.Wild! Profound implications for clinical practice and the foundational models of hepatobiliary diseases!
-
@CrumblingCookie there is a study showing pancreatic cancer patients usually have a fungal infection of the pancreas
and secondly, there is a case report of elevated liver enzyme ALP going down after anti fungal treatment in suspected fungal infection. this is with the generally liver toxic anti fungal drug.
-
@sunsunsun Yes, yes! The clinical neglect and snotty obfuscation into esoteric quackery is maddening!
Will update soon on what I'm doing.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login