Testicular microlithiasis (calcium deposits) and atrophy
-
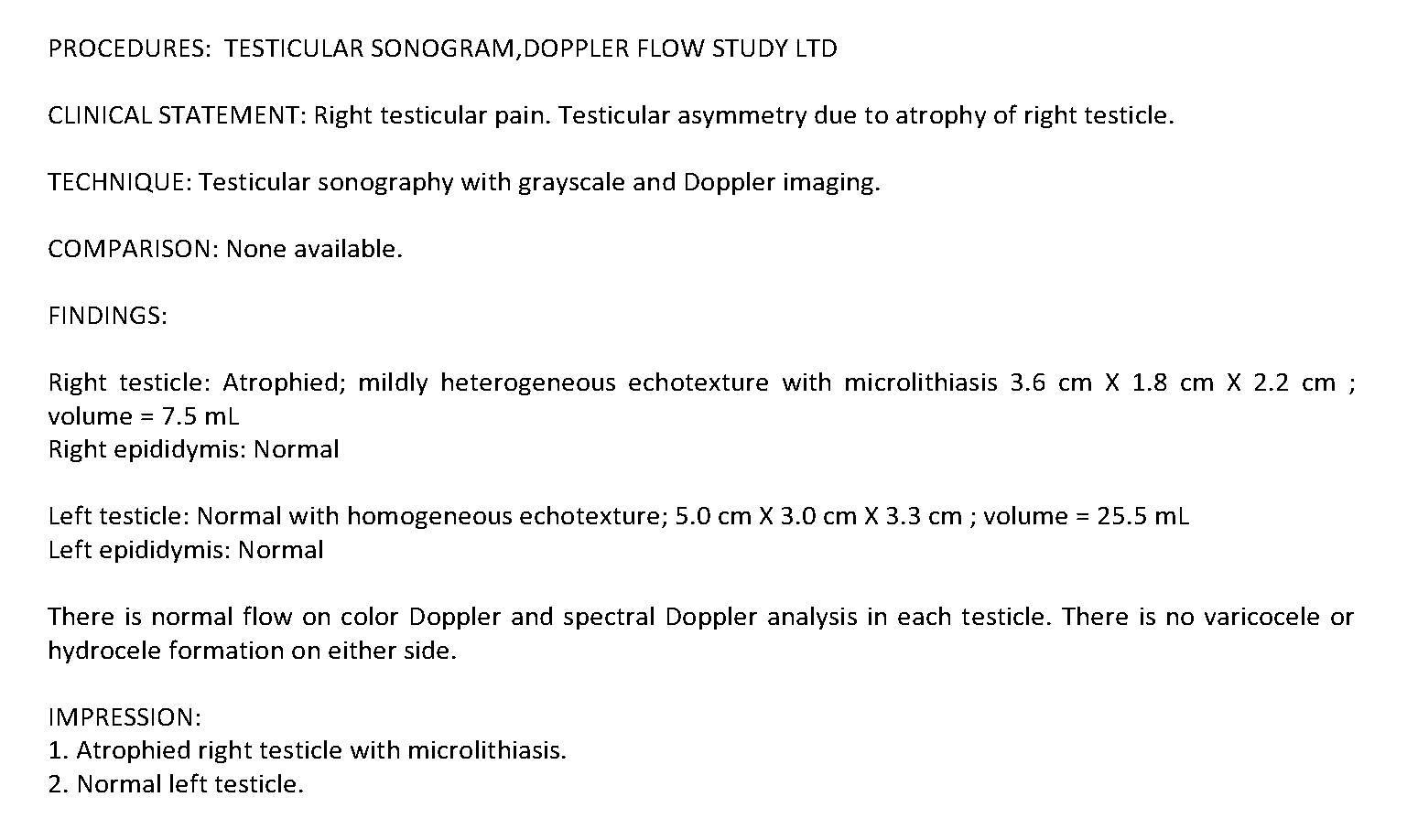
My right testicle has atrophied (shrunken) and an ultrasound this week revealed microlithiasis—small calcium deposits—on that side. Doc said not a lot is known about this and just recommended an annual ultrasound and monthly self-checks to monitor for changes.
I'd like to address it. I first noticed that the right testicle had shrunken a bit about two years ago but it seemed within normal range so I didn't think much about it. I figured it was maybe a varicocele or something and made a few efforts at alleviating that (pelvic exercises, etc.). The left testicle has been normal throughout although I think it has grown a bit, possibly to compensate for reduced function in the right. Here are the ultrasound results:
I have a fairly high-calcium diet and take a few thousand IUs of d3 every morning and a mg or 2 of Kuinone most evenings. I use topical magnesium for deodorant and occasionally mix up some mg bicarbonate to drink. As I understand it, these substances are major factors in calcium regulation/deposition.
Some more background in case it's helpful:
- Have been into Peat/bioenergetics for about 3 years
- Diet is typical: coffee w sugar and milk in throughout morning to early afternoon, lots of fruits, orange juice, haagen dazs, potatoes, mushrooms, occasional rice, beef and lamb, shrimp, weekly dozen oysters and liver
- Only supplements are D3, K2, occasional Thorne Ultimate-E, occasional aspirin and baking soda. I was taking some topical androsterone to help with mild gyno recurrence but stopped because it wasn't doing anything.
- Labs are mostly fine I think. TSH is 1.1, slightly elevated cholesterol. You can look at bloodwork history here if you want, including results from last week. CO2 is a little lower than I would expect, and calcium is at the high end of the reference range.
- I had T and Free T, and prolactin measured about six months ago. T was 581, Free was 13.1, and prolactin 8.7. The T numbers, especially Free T, are lower than I expected. Lately I have noticed thinner hair on the back of my calves which is a symptom of declining testosterone, so I will probably have this re-measured in the next week or so.
Really any advice is helpful. I've found very little information about this condition online and I am pretty freaked out about it.
-
The blood calcium level seems a bit on the higher end. This is usually regulated by Parathyroid hormone. Not sure if you've ever had PTH levels checked. Also the Vitamin D level (22.2, not sure of the units) seems a bit low. Maybe it has come up in the past three years with your supplementation, but maybe not.
That said, I'm not sure if that's related to your issue.
-
@Crypt-Keeper Will add PTH to my labs this week, good call. And yeah, probably not a bad idea to check D levels as well…I wasn't supplementing at all when that measurement was taken.
-
@chateau_marmot I know Chris Masterjohn recommends getting the below tests taken together. (These are LabCorp names so might be different for your lab.)
Ca+PTH Intact (this is basically Calcium and PTH, Intact)
Calcitriol(1,25 di-OH Vit D)
Vitamin D, 25-HydroxyHe has ways of drawing some conclusions from those.
Is your hair thinning yet?
Here is the LabCorp interpretation. I doubt you have a PTH problem but there might be something there that can be optimized.
Interpretation Intact PTH Calcium (pg/mL) (mg/dL) Normal 15 - 65 8.6 - 10.2 Primary Hyperparathyroidism >65 >10.2 Secondary Hyperparathyroidism >65 <10.2 Non-Parathyroid Hypercalcemia <65 >10.2 Hypoparathyroidism <15 < 8.6 Non-Parathyroid Hypocalcemia 15 - 65 < 8.6 -
@Crypt-Keeper Thanks this is really helpful. Hair is slightly thinner near hairline than it used to be, yes.
-
@chateau_marmot - I like the suggestion to look at your PTH level. Dr. Peat recommended a dietary ratio of calcium to phosphorous of at least 1.1 to 1 to keep your PTH in range. If your concern is calcium deposits in your soft tissue, it will seem counterintuitive to encourage you to increase your dietary calcium. But that may be what you have to do. I suggest that you use an app like cronometer.com and look at your dietary ratio for a few days.
I asked Peatbot.com:
pth and calcium deposits?Peatbot: Parathyroid hormone (PTH) plays a crucial role in regulating calcium levels in the blood and bone metabolism. When PTH levels are high, it can lead to various issues, including the inappropriate deposition of calcium in places other than the bones, such as soft tissues and arteries.
PTH is secreted by the parathyroid glands and is primarily responsible for maintaining the calcium concentration in the blood. It does this through several mechanisms:
-
Bone Resorption: PTH stimulates osteoclasts, which are cells that break down bone tissue, releasing calcium into the bloodstream.
-
Calcium Reabsorption in the Kidneys: PTH reduces the amount of calcium excreted in the urine by increasing the kidneys' reabsorption of calcium.
-
Activation of Vitamin D: PTH stimulates the conversion of vitamin D into its active form, calcitriol, in the kidneys. Calcitriol, in turn, increases the absorption of calcium from the diet in the intestines.
However, when PTH is chronically elevated, it can lead to excessive mobilization of calcium from the bones, which can contribute to osteoporosis—a condition where bones become weak and brittle. Additionally, high levels of PTH can cause calcium to deposit in soft tissues, including the arteries, leading to calcification and associated complications such as atherosclerosis.
The context provided explains that the excess phosphate intake can trigger the parathyroid glands to release more PTH, which then causes calcium to be mobilized out of the bones and into the bloodstream. This process is exacerbated by the presence of lactic acid, which shifts the pH of the cells and promotes the formation of insoluble calcium phosphate crystals in the mitochondria of cells. As the mitochondria die, these crystals can accumulate in soft tissues, contributing to inflammation, degeneration, and immune failure.
To connect high PTH levels with these issues in a clinical setting, a blood test showing a low vitamin D content could be an indicator, as vitamin D helps to balance calcium and phosphate in the body. Additionally, a high Thyroid Stimulating Hormone (TSH) level and aldosterone, part of the angiotensin system, are associated with PTH activity.
In summary, PTH is essential for calcium regulation, but when it is chronically elevated, it can lead to the loss of calcium from bones and the deposition of calcium in soft tissues and arteries, contributing to various health problems.
I hope this helps.
-
-
lowering parathyroid hormone:
-increase calcium
-increase vitamin d
-increase magnesium
-caffeine
-famotidine -
To the OP, i'll recommend that you also research Boron to see if it can fit into your puzzle. It ties in with a couple of different aspects being discussed here.
I'll stress researching it first before adding it to a daily stack. There are some potential cons to be aware of and it's a mineral that we need very little of, with breaks taken from it during the week even. There's some research material here and plenty more at the other forum of course.
-
Appreciate everyone's insights. I'm going to start by getting the following tests this week and will update this thread as things progress in case it can be useful to others.
- PTH + Calcium
- Calcitriol
- Vitamin D 25-hydroxy
- Free testosterone
- Total testosterone
- LH + FSH
- SHBG
-
Today, Dr. Mercola posted an article echoing Dr. Peat's recommendation.
How Your Calcium-to-Phosphorus Impacts Your Health
STORY AT-A-GLANCE
Many people have an imbalanced calcium-to-phosphorus ratio (Ca:P), consuming high levels of phosphorus and low levels of calcium, which can be detrimental to optimal health
Western diets typically provide ample phosphorus due to high levels in meat, grains, beans, and processed foods, but often lack sufficient dietary calcium
An ideal Ca:P ratio is close to or above 1:1; however, many popular diets, including dairy-free and carnivore diets, often result in ratios well below this, such as 0.3:1
Inadequate dietary calcium can lead to the body mining calcium from bones and teeth, and maintaining elevated parathyroid hormone levels, which are associated with systemic inflammation and accelerated aging
Simple dietary adjustments, like tracking nutrient intake through apps and adjusting food choices, can help restore a balanced Ca:P ratio -
@chateau_marmot do you have calcium deposits under your eyes too? or under eyebrows
generally it can be a sign of not enough thyroid hormone functioning (needed to deal with calcium in cells,
calcium buildup can indicate cells are dying in mass at that area (i,e possibly not enough glutathione / catalase protection against your toxin burden, poor mitochondria function due to hypothyroid, chronic inflammation in an area -
@cs3000 Hmm…I don't think I do now but looking at pictures I think I definitely used to have them under my eyes.
when cells die they are calcium overloaded, indicates cells are dying in mass at that area
This is helpful, sounds like the microlithiasis is likely a post-atrophy symptom.
Very strange to me that this has only happened on one side. Doctors said there is no indication of an injury or infection that might have caused the atrophy so I'm a bit in the dark as far as determining a cause.
How can I increase glutathione/catalase protection?
-
@chateau_marmot
is it the same side where you put your phone into a pocket if u do that regularly?idk how far it could help specific to your situation but alpha lipoic acid might be worth researching https://pubmed.ncbi.nlm.nih.gov/33529370/ https://www.sciencedirect.com/science/article/abs/pii/S0890623824000224
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3823291/
and theres a thread here on ergothionine -
@cs3000 It is… I try not to anymore but I did for a long time.
Thank you for the links, will dig into it
-
@Chud said in Testicular microlithiasis (calcium deposits) and atrophy:
-increase vitamin d
-increase magnesiumVitamine D : https://vitamindwiki.com/One+pill+every+two+weeks+gives+you+all+the+vitamin+D+most+adults+need
Magnesium : https://vitamindwiki.com/Overview+Magnesium+and+vitamin+D -
Quick update: LH and FSH labs came in.
FSH seems normal at 7.7mIU/mL (range is 1.5–12.4)
LH is quite high at 9.0mIU/mL (range is 1.7–8.6)
Current hypothesis is that the microlithiasis is a result of atrophy and not a cause (ruling out calcium regulation issue unless PTH/calcitriol labs come back abnormal).
I also think that the high LH indicates primary hypogonadism rather than secondary.
Still in the dark about a cause, however. The fact that it's only one testicle seems very bizarre. Going to get in with a good urologist to see if they can tell me more. I'll also ask the radiology lab for the ultrasound images and post them here.
In the meantime—any pointers on lowering LH are welcome. I've read that high levels in the blood cause aromatization so will try to ameliorate that.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login