Random, interesting studies
-
@Mauritio said in Random, interesting studies:
@dapose said in Random, interesting studies:
I’m using Boswellia every night before bed with baking soda and glycine water. Most consistent vivid dreams I’ve had as an adult!
It’s a COX enzyme blocker, very good anti inflammatory for me.Nice! Do you notice any hormonal or metabolic effects from it ?
Nothing too specific on hormonal or metabolic front. But I’ve gone on and off Boswellia a few times and it without a doubt makes dreams more vivid and way more memorable for me.
A side not… I recently started taking Gonadin by Idealabs (first time and for about a week) I read every single comment on the old RPF for Georgi’s thread and I saw your name pop up a few times in that thread. Did you like taking Gonadin? Are you still using it to any regularity? And specifically the newest version of it…
peace! -
@dapose I started taking frankincense too. The range of benefits is just too wide to ignore.
I don't take Gonadin anymore. I think the old one was better and had some really interesting chemicals like Diosgenin or phytol in it.
The new one makes me robotic.Dare to think.
My X:
x.com/Metabolicmonstr -
@Mauritio yeah it seemed from that long thread that everyone was liking phytol and had definite productive responses to it… couldn’t tell why that needed to be changed. I’ll see how the new one goes. I really like the taste of the passionflower extract azf.
-
500mg/KG BW sodium citrate (SC) is about equally effective as 300mg/KG BW sodium bicarbonate (SB) in raising blood pH and blood HCO3- in healthy people.
The increase in the SC group however took about 1h longer to set in and also lasted for longer than the SB:
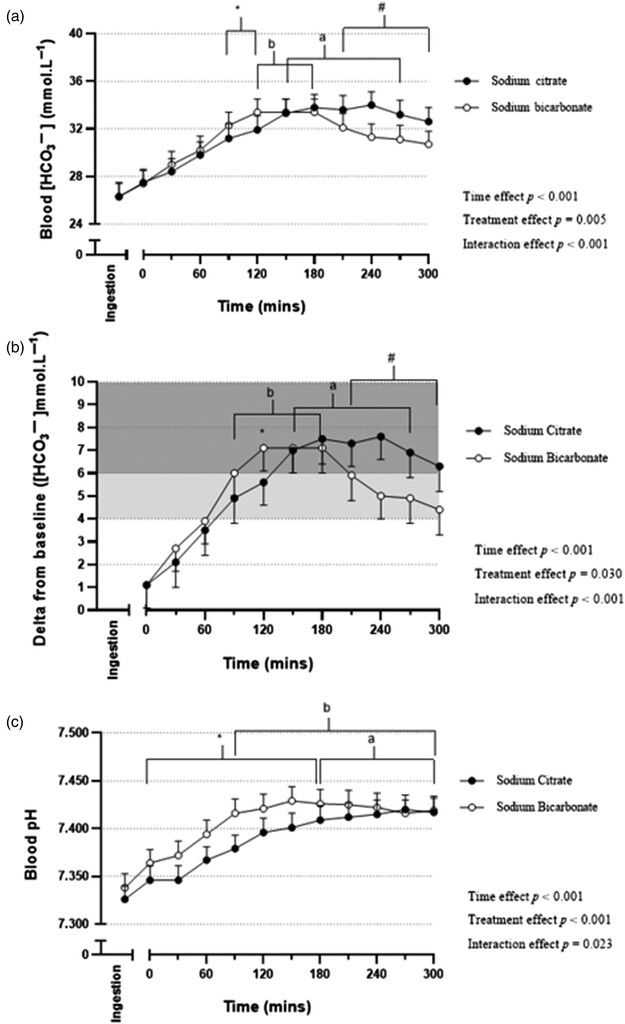
I'd say give the citrates a try for simplicity although in this study, the gastrointestinal side effects/complaints were comparable between SC (~35g!) and uncoated SB (~21g!).
Whilst the SC also does meddle with stomach pH, it won't react to CO2 (burping, flatulence).
The release of HCO3- from citrate happens indirectly through liver tricyclic-acid metabolism.And of course use potassium citrate or a citrates blend instead of the sodium salt.
@mossy @ena There are several online suppliers of potassium citrate capsules (~1110mg per capsule, whereof 400mg K) as an affordable alternative to buying the pure powder and dissolving a teaspoon in water two times a day.
10grs of potassium citrate contain about 3.6grs K, 10grs of potassium bicarbonate ~3.9grs K.
Although the same amount (by weight) of citrate is not as effective as bicarbonate, on a regular daily basis I think one can shift between using either. -
Thank you @CrumblingCookie. Good information. But I see no financial advantage in citrate, here in the UK potassium citrate powder costs £14/kg and potassium bicarbonate £4/kg.
-
Protective Effects of Ginger against Aspirin-Induced Gastric Ulcers in Rats
-
Phytol
Phytol lowers weight gain on a HFD. Drastically increases UCP1 (by 10x in white adipose tissue!), PGC1a and AMPK. It also strongly increases the most important enzyme for glucose oxidation, Pyruvate dehydrogenase (PDH).
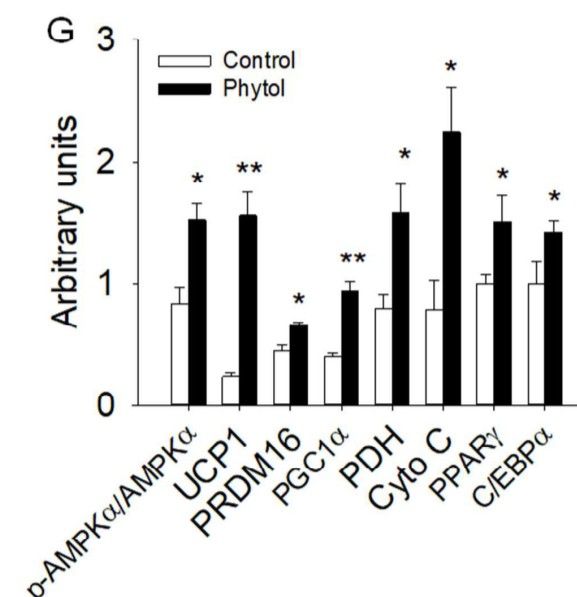
https://sci-hub.ren/10.1039/C7FO01817G
"...PHY efficiently interacts with COX-1 and 2, NF-κB, and IL-1β. In conclusion, PHY exhibits anti-inflammatory activity, possibly via COX-1 and 2, NF-κB, and IL-1β dependent pathways."
https://pubmed.ncbi.nlm.nih.gov/32583784/
Phytol, Produces Antihyperalgesic, Anti-inflammatory, and Antiarthritic Effects
https://pubmed.ncbi.nlm.nih.gov/32091204/
Phytol seems to be a GABA-A receptor agonist, lengthening sleep time
https://pubmed.ncbi.nlm.nih.gov/39357640/
Again, it binds to GABA-A receptor, but also to 5HT1A. Not sure if it agonizes or antagonizes it.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11926570/
Phytol drastically inhibits gastric ulcers
https://pubmed.ncbi.nlm.nih.gov/38717706/
Could be a dopamine d2 antagonist based on its antiemetic properties. But could also be due to possible 5ht3 antagonism (similar to ondansetron) .
https://pmc.ncbi.nlm.nih.gov/articles/PMC10008523/
Anti-bacterial effect / anti-biofilm
https://pubmed.ncbi.nlm.nih.gov/27667264/
https://pmc.ncbi.nlm.nih.gov/articles/PMC5723315/
In Vitro Anticancer Activity of Phytol on Human Non-Small Cell Lung Cancer A549 Cells
https://pubmed.ncbi.nlm.nih.gov/40468754/
Phytol lowers inflamamtion (paw edema) induced by serotonin or histamine.
It also lowered inflammatory cytokines and MDA and increased glutathione. The effect was dose dependant.
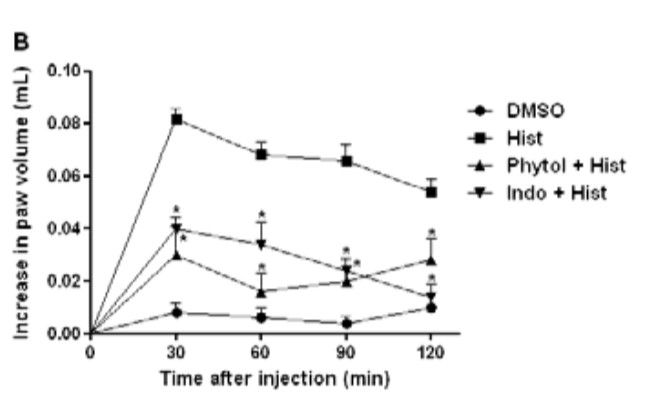
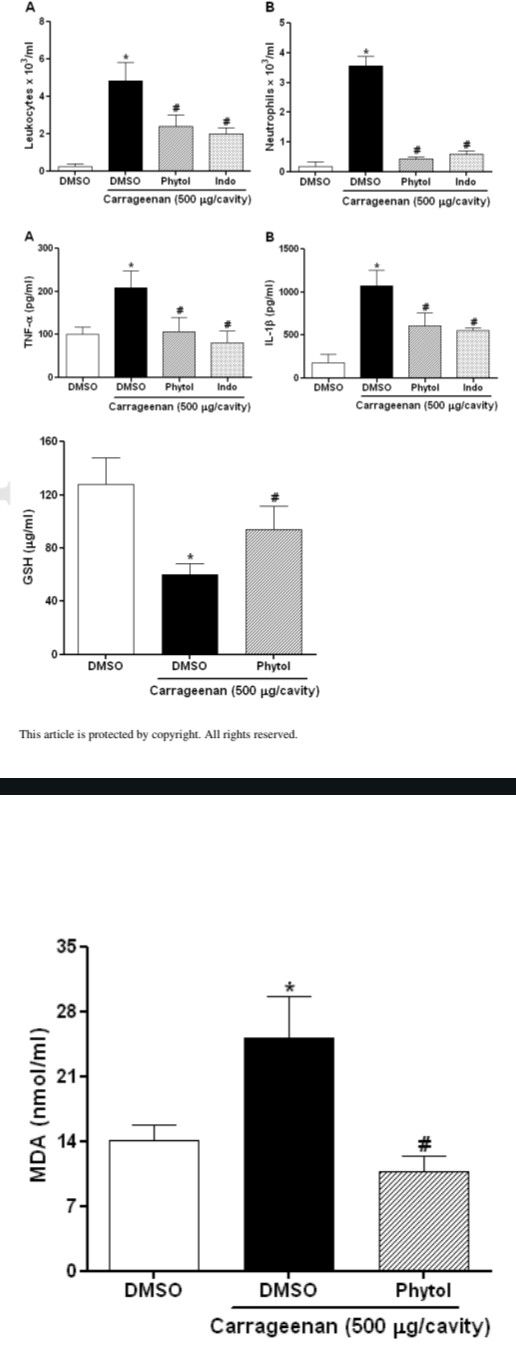
https://sci-hub.ren/10.1111/fcp.12049
BTW Haidut posted studies on phytol increasing progesterone and testosterone synthesis. The optimal dose was an HED of around 0.8mg/kg
https://lowtoxinforum.com/threads/archive-info-for-old-gonadin-version.43485/
Haidut also posted this study which shows that phytol inhibits an enzyme thst leads to lower NAD levels. So they showed that giving mice phytol increased blood NAD levels.
https://pubmed.ncbi.nlm.nih.gov/23832361/It's a completely different pathway compared to what is usually used to manipulate NAD levels.
This enzyme is mostly expressed in liver and kidneys.
In studies it was shown that inhibitiing this enzyme reversed NAFLD and acute kidney injury!
https://pmc.ncbi.nlm.nih.gov/articles/PMC11741923/ -
Lemon balm / Melissa
Anti-estrogenic:
anti-cancer effect against breast cancer . Most effective against estrogen sensitive breast cancer.
https://pubmed.ncbi.nlm.nih.gov/32351599/It decreases the severity of dismenorrhea, again pointing towards an anti-estrogen effect.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6447884/Decreases symptoms of PMS.
https://pmc.ncbi.nlm.nih.gov/articles/PMC4557408/Anti- prolactin/Anti-TSH:
https://pubmed.ncbi.nlm.nih.gov/7202226/
Lowers weight gain on a HFD. Lowers FFAs and triglycerides.
https://sci-hub.ren/10.1016/j.jep.2020.113360
Thyroid:
It seems to be the common opinion that lemon balm is anti-thyroid. The studies that I've read only point towards it being anti-TSH. That's a difference. Peat was against TSH.
"TSH has direct actions on many cell types other than the thyroid, and probably contributes directly to edema, fibrosis, and mastocytosis."
I found a study where they induced hyperthyroidism and indeed lemon balm did lower thyroid hormones - but only in the hyperthyroidism group. Not in the group that only received lemon balm. As you csn see below, in normal animals it had basically no effect on thyroid hormones (MO group).
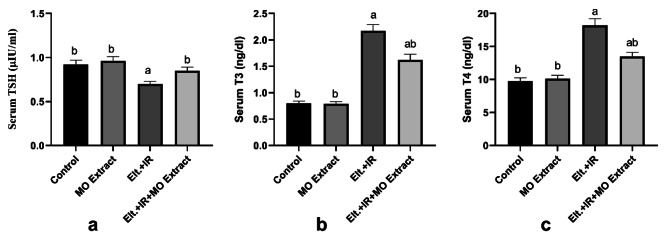
https://pubmed.ncbi.nlm.nih.gov/2985357/ -
Androgenic and aphrodesiac action of the medicinal plant Lithospermum Arvense (bird millet)
-
@Mauritio wow nice! And Lemon Balm is super easy to grow perennial herb. Available in most garden stores. Smells great too!
-
@Mauritio do you mess around with any phytol these days? Food or extract… is there a supplement phytol? Or just load up on the skins of nuts and slam seaweeds?

-
@dapose said in Random, interesting studies:
And Lemon Balm is super easy to grow perennial herb. Available in most garden stores. Smells great too!
Yes. And I haven't even posted all the cool studies on it . There's more for dopamine, liver health and as an anti-viral.
I've been taking lemon balm extract for over a week. And i finally feel like I'm not about to catch a cold for the first time this winter. It's also very calming and seems to help weight loss. Seems to lower blood sugar noticably. -
@dapose said in Random, interesting studies:
do you mess around with any phytol these days? Food or extract…
Ive ordered a food grade phytol supplement from Spain. Some herb, weed or terpene shops carry it.
I'm looking forward to trying it.Im kinda trying to recreate the 1/2nd generation Gonadin.I already take Diosgenin, now phytol . Next methyl oleate (might be able to accelerate PUFA detox).
-
Rose hip
Rose hip increases thermogenesis, browning of white adipose tissue and UCP1 (a lot)
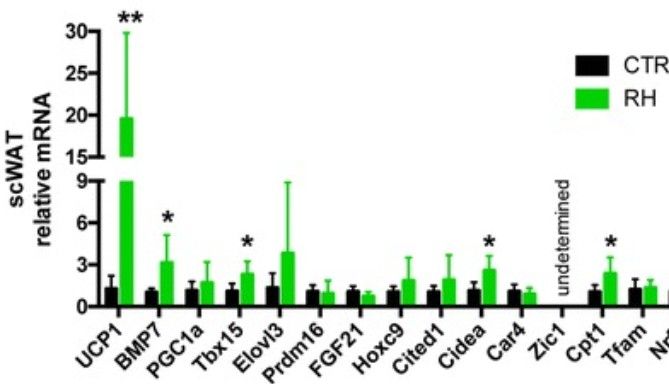
https://pubmed.ncbi.nlm.nih.gov/27980600/Rose hip extract lowers weight gain on a HFD, lowers visceral and liver fat.
https://pmc.ncbi.nlm.nih.gov/articles/PMC3892499/It reduces atherosclerosis,oxidized LDL, total cholesterol and fibrinogen.
https://pubmed.ncbi.nlm.nih.gov/28399420/Daily intake of rosehip extract decreases abdominal visceral fat in preobese subjects
https://pmc.ncbi.nlm.nih.gov/articles/PMC4358417/#sec15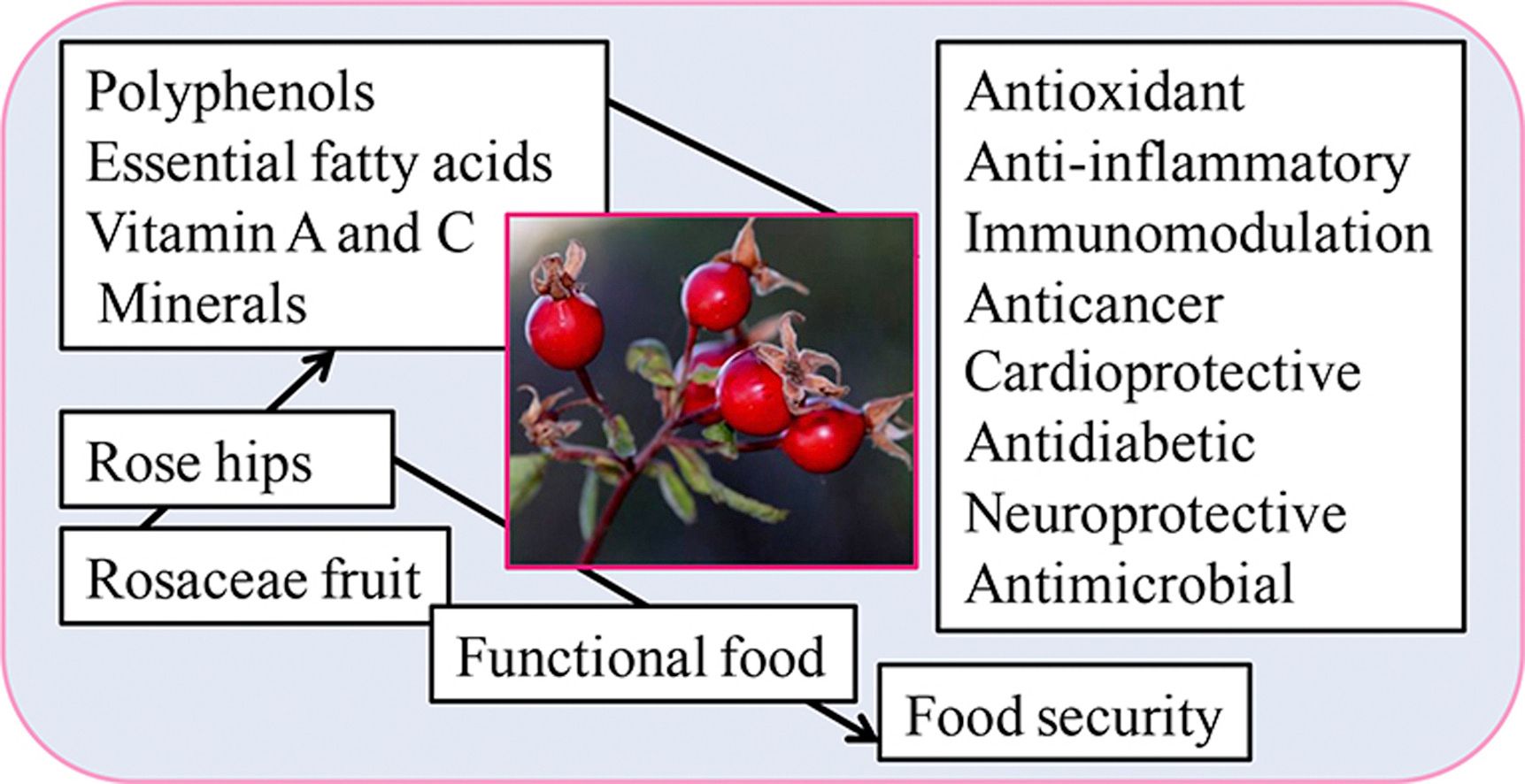
https://www.sciencedirect.com/science/article/abs/pii/S0924224416304277 -
@Mauritio
From Wikipedia, the free encyclopedia
Phytoprogestogens, also known as phytoprogestins, are phytochemicals (that is, naturally occurring, plant-derived chemicals) with progestogenic effects.[1][2]Relative to their phytoestrogen counterparts, phytoprogestogens are rare.[1] However, a number have been identified, including kaempferol, diosgenin (found in yam), apigenin (found in chasteberry),[1][3] naringenin, and syringic acid, among others.[2] In addition, 3,8-dihydrodiligustilide from Ligusticum chuanxiong is a potent progestogen (EC50 = 90 nM), whereas riligustilide is a weak progestogen (EC50 ≈ 81 μM).[4][5]
carrot salad by R.Peat delivers apigenin (phytoprogestogen) and absorbs estrogens
https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2024.1359176/full
" In mice, NAD+ levels can be elevated via treatment with apigenin, a natural flavonoid that inhibits the NAD+-consuming glycoprotein CD38."
Progesteron synthesis depends on NAD as a cofactor as well as myo-inositol synthase . -
@cedric said in Random, interesting studies:
From Wikipedia, the free encyclopedia
Phytoprogestogens, also known as phytoprogestins, are phytochemicals (that is, naturally occurring, plant-derived chemicals) with progestogenic effects.[1][2]Yes I have posted this very paragraph in this thread before. Not sure how strong Diosgenins progestogenic effects are, it feels more androgenic.
I have posted about syringic acid and the Chinese herb progestogen as well.
-
-
@Mossy I really liked the effects it did worsen sleep though.
-
@Mauritio @mossy i had a cup of lemon balm tea after lunch yesterday and it was very calming, similar to chamomile but not sleepy-calm. My guess is that lemon balm is better for day time stress, and chamomile better for after dinner nighty night time! 🫖

-
Vitamin K2 Protects Against Glucocorticoid-Induced Osteoporosis by Activating the NRF2/FSP1 Pathway to Inhibit Osteoblast Ferroptosis
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login