Bile can serve as a reservoir for funghi, making them harder to treat
-
@sunsunsun said:
any opinion on pH and yeasts?
Which pH where are you thinking of?
I'd confidently say that high stomach pH is a very significant risk factor.
Especially over time.
Not only is there a higher quantity of yeasts passing the stomach but also the less acidic chymus will be met by less alkalic bile (or lesser quantities thereof).
Unless there's some metabolic bicarbonate depletion (on top) which puts the less alkalic bile into first place of such chicken-egg interdependencies.
Any way, there'll be more exogenous microorganisms than there ought to be and along with the incomplete digestion and shifts in microbiome more mucosal disturbances and pathogenic colonization and translocation.
I've come across this publications from 1965 on moniliasis (=candidiasis) Moniliasis, Steatorrhea, Diabetes Mellitus, Cirrhosis, Gallstones, and Hypoparathyroidism in a 10-Year-Old Boy and found it interesting how they (unsuccesfully) discussed the very confusing and complex relations.
They had probably stumbled upon the back then still unestablished "Autoimmune Polyglandular Syndrome Type 1 (APS-1) / Autoimmune Polyendocrinopathy-Candidiasis-Ectodermal Dystrophy (APECED)".
Yet I don't know whether such a term and associated genetic variance has resolved any underlying mechanisms.
They were really confused as to what's causing what.
What they observed were strongly reduced magnesium uptakes (probably because of fungal infection), which is necessary for parathyroid hormone synthesis, followed by accordingly diminshed calcium uptake. D3 was of no assistance. There was also lots of steatorrhea which preceded many of the other symptoms by years and is somehow reciprocally dependent on calcium. And autoimmunity (intracellular fungal vacuoles? antibody or T-cell cross-reactivity? antigenic mimickry?) against the (para)thyroid gland, as well as hepatic changes. A real mess!-> I'm suspecting that any mess with having both decreased magnesium yet also decreased/intolerable Mg uptake and a chronically fluctuating/insufficent calcium metabolism should point oneself to consider fungal infections! It surely won't be as extreme as in those genetic cases but how would you ever know whether PTH levels are as high as they need to be?
Disturbances of these essential alkaline electrolytes sort of lead back, over a long stretch, to your general pH question.
Pertinent to the discussion may be work presented by Louria and Brayton in Nature (Jan. 18, 1964, p. 309), who found a substance in blood lethal to Candida albicans in normal persons. A moderate to marked reduction to this substance was found among patients with cirrhosis, hepatitis, diabetic azotemia, and in patients with mucocutaneous and systemic moniliasis.
The percentage of persons possessing the factor is slightly reduced among groups of patients with diabetes (without azotaemia) and with disseminated carcinoma.
This is about transferrin again @sunsunsun .
Specifically, back then they had narrowed it down to a molecule between 10-20kDa - which surprisingly doesn't match up with transferrin but suggests an even more potent polypeptide that has been split off the complete transferrin molecule. Unless their filter meshes back then were somehow wrong. Anyway the results of the other studies suggest that transferrin is a direct source of this active polypeptide.The substance appears to have impressive specificity. It is active against Candida albicans and Candida stellatoidea but not against other Candida species [glabrata, krusei] or other yeasts such as Cryptococcus neoformans or Saccharomyces cerevisae.
! The iron-chelating property of this likely transferrin peptide does not harm C. glabrata or C. krusei or other non-albicans fungi! This is highly relevant.
Puts the approaches directed at iron-chelation also in a highly species-specific context to consider.
Tannic acids are highly anti-fungal. Among other mechanisms, they inhibit hyphal growth of C. albicans and hinder their adhesion to mucosal cells. In animal experiments, sufficient dietary tannic acids directly increased Candida excretion (i.e. fungi which failed to colonize or invade).This may be an important mechanism behind the acutely anti-diarrheal and anti-microbial activities of oral tannin-albuminate or tannin-gelatinate.
Sort of shifts the dietary focus away from those merry-go-round prebiotic and soluble or insoluble fiber discusstion and puts weight onto dietary tannic acid content. Which also lead to fruit (berries!) and vegetables and rather more traditional, more natural, tarter or more bitter varieties than today's varieties aimed at maximizing sweetness and yield.
One of the most widespread and available tannins which also offers large mucosal absorption is EGCG.
EGCG of course strongly chelates iron. Surprisingly, though, it provides a more complex mechanism of action.
EGCG is indeed most antifungal against C. glabrata! EGCG sort of also targets liver tissues so this is good news.
Have ordered EGCG (decoffeinated) to augment the FCy/5-FC and horseradish.
Some flavonoids markedly downregulate Candida CDR1 (which regulates the efflux pumps and resistances against azoles!):
Flavones, Flavonols, and Glycosylated Derivatives-Impact on Candida albicans Growth and Virulence, Expression of CDR1 and ERG11, CytotoxicityThe reduction of both fungal virulence and expression of antifungal resistance-linked genes was the most pronounced for apigenin and apigetrin; these results indicate flavonoids' indispensable capacity for further development as part of an anticandidal therapy or prevention strategy.
Here, however, kaempferol's antifungal properties beat apigenin, which exhibits some ambiguous and controversial effects (like upregulating ERG11, inhibition of which is the target for azoles) by miles. Kaempferol seems worth noting down.
Inhibition of Candida albicans extracellular enzyme activity by selected natural substances and their application in Candida infection, 2008 -
@LucH said in Bile can serve as a reservoir for funghi, making them harder to treat:
Thank you for the detailed answer.


And Yes, retinol is also required in the immune process (interaction with A D K). I take 2x/wk. 5 000 UI (retinyl palmitate).
So, you obviously don't think the vitamin A from liver is enough or effective in the same manner as supplementing vitamin A? If AI is correct, it states: "A 4-ounce serving of beef liver contains approximately 9,000 to 25,000 IU of vitamin A, while chicken liver has around 13,000 to 16,000 IU."
"To desire action is to desire limitation" — G. K. Chesterton
"The true step of health and improvement is slow." — Novalis -
@CrumblingCookie said in Bile can serve as a reservoir for funghi, making them harder to treat:
I wouldn't know! I dislike and distrust liver so have gone for the isolated substances and followed them up with testing of serum (free) copper, ceruloplasmin and retinol. IIRC there was one guy writing on the old RPF that he had eaten lots of liver regularly and his lack of copper was surprisingly unaffected until he started supplements.
Ok, I can appreciate that perspective. I don't like the taste of liver. I take it purely as a medicine. I only eat 2 oz at a time now, because I dislike the taste so much. When I used to eat 4 oz, I could feel the positive effect it had on me. Sometimes with the 2 oz, but not as much.
"To desire action is to desire limitation" — G. K. Chesterton
"The true step of health and improvement is slow." — Novalis -
@Mossy said in Bile can serve as a reservoir for funghi, making them harder to treat:
you obviously don't think the vitamin A from liver is enough or effective in the same manner as supplementing vitamin A?
No. Whenever I can eat 2 chicken livers (broth) it's fine. Not always available.
No need to supplement if I eat liver.
Apart case: Infection, higher ratio and more D3. -
@Mauritio Any new ventures into this? I've seen in your other threads that you've been harbouring fungal suspicions for a very long time.
Your mentioning of molybdenum to potentially counter any initial fungal "die-off" symptoms made me wonder if those dogmatic followers on the LTF are also actually onto chronically persisting fungi with all their EGCG megadosing. Thoughts?
Mo doesn't seem to help me.
EGCG absorption is quite low and it's highest on an empty stomach after fasting.
So I'm moving the complete daily dose to the morning instead of having it split up, so it can reach at least inhibitory concentrations in the body. 1050mg EGCG pd.Have also started the horseradish and nasturtium powders throughout the day. 3,000mg nasturtium and 1,200mg horseradish pd.
When I open the capsules, however, they don't taste very pungent at all in my mouth. Only very slightly and super-transiently. Gone after 10 seconds. 1.2g of ground, dried horseradish also sounds very little. I probably should be taking four times as much per day, as 1.2g would only be about 8g of fresh horseradish. I didn't get a brand product because of the nasty tablet fillers so there could be further variances in the raw products and drying process.
Perhaps an appropriate amount of benzyl-ITC could indeed be better?Peak serum levels of FCy (5-FC) at my 95mg/kg dosage are still unknown to me after two weeks of administration - which really isn't ideal. Hopefully they're high enough to be therapeutic.
So far there's not a hint of hematological / bone marrow suppression. CBC is as fine as always.In summary:
I'll continue now every day with FCy 95mg/kg, EGCG 1050mg, dried nasturtium/horseradish 10g/4g, UDCA 500mg. And the aforementioned probiotics, few B vitamins, colloidal silicium.
And I'm now going to start artichoke leaf extract, equivalent to 4g - 12g of raw artichoke leaf, 3-4x daily. Predominantly for increasing hepatic bile synthesis and output. If it inhibits and decreases hepatic cholesterol synthesis and storage that should theoretically assist.
I had the oregano essential oil and garlic slip. Either my initial garlic bulbs were very weak and the Chinese garlic bulbs I have now are hugely more pungent or I have grown tired of it, or both. -
@Mossy chicken liver is actually scrumptious when prepared via my world-famous bbq baked bean and chicken liver recipe. I dont exactly like eating fried liver and onions plain other than on the rarest occasions, and even then I have to chase it with mashed potatoes, ketchup, and an ice cold Coca Cola, but the chicken liver and bbq baked beans recipe I have is fire af on buttered bread, lmk if u want it, it's easy to make with canned baked beans too. it actually gets better in the fridge a day or two after cooking it too.
-
@sunsunsun let us know
-
C CrumblingCookie referenced this topic on
-
@CrumblingCookie said in Bile can serve as a reservoir for funghi, making them harder to treat:
Any new ventures into this?
Yes, I'm trying TUDCA atm.
It's interesting that some bile acids have pro-microbial effects (primary BAs) and some have anti microbial effects (secondary BAs).
https://pubmed.ncbi.nlm.nih.gov/39204302/TCA for example enables fungal infections.
"...TCA through drinking water is sufficient to induce colonization and dissemination of CA in wild-type and immunosuppressed mice."
https://pmc.ncbi.nlm.nih.gov/articles/PMC8708873/While LCA and DCA have anti-fungal effects in a variety of ways. (TUDCA should have a similar effect)
"Interestingly, LCA and DCA also significantly inhibited the germ tube, hyphae and biofilm formation in C. albicans. "
https://pubmed.ncbi.nlm.nih.gov/29648597/
The main reason for taking tudca is to thin the bile and support the liver - gallbladder axis. That seems to be the bottleneck for me.
Maybe working on the affected organs is more fruitful than trying to eradicate the fungus? Not sure.
And since TUDCA should have significant direct anti-fungal effects on top of that, it could be suitable candidate in my case. -
@Mauritio It's difficult to do without cholic acid as the most crucial primary bile acid... the conjugated bile acids are protective to fungi yet the unconjugated CA allegedly isn't.
Perhaps this requires to temporarily dial back on any supplemental glycine and taurine in case of fungal issues?
UDCA and TUDCA appear to be rather neutral towards fungi from what I can find.I'had looked into therapeutic DCA use as well but it's also strongly cytotoxic to human cells. Or perhaps I'm not remembering correctly and endogenous DCA abundance is always being mixed up with a concurrent abundance of the more harmful LCA.
Any way, DCA is tough to get if. I couldn't. Maybe straight from Asia. Supplementation was propagated by a medical practitioner from Eastern Europe who went on to sell the raw powder directly but eventually even that has become suppressed. It used to be available as a pharmaceutical raw material but that has been utterly stomped whilst at the same time it's still classified as a pharmaceutical so it's illegal to import.
Still available for lab and research use, however, if you can buy it via a certifiably appropriate company.
Obfuscations and intransparancies everywhere one goes or looks.Peak serum levels of FCy/5-FC came in just under the therapeutic optimum.
Therefore raising it to 118mg/kg BW for the last week which by linear extrapolation should push peak serum levels up to a solid 62 µg/mL.@Mauritio said in Bile can serve as a reservoir for funghi, making them harder to treat:
The main reason for taking tudca is to thin the bile and support the liver - gallbladder axis. That seems to be the bottleneck for me.
In the past I had notable success with that, but not anymore. A mild version of the "liver/gallbladder cleanse" olive oil/grapefruit juice blend but without the Mg-SO4 really unclogged things and whilst gentian and taraxacum are the basic cholagogics I believe tincture of gold coin grass aka Lysimachia aka Jin Qian Cao or glechoma hederacea was a profoundly effective addition back then, too.
-
@CrumblingCookie have you tried high dose riboflavin , and niacinamide?
also there’s a new antifungal out called brexafemme , that is the brand name. the drug name starts with an i.
-
@sunsunsun
Hi. Yes I had repeatedly tried high-dose riboflavin, up to gram dosing.
Also tried niacinamide throughout the day in mid or in high dosing.Had read your old thread on the RPF again on riboflavin activity against Candida. Unfortunately, there are crucial caveats to it: That only applies to C. albicans.
C. glabrata, however, thrives on it. Throwing B2 or B1 or B3 at C. glabrata acts as a strong growth stimulant. C. glabrata (and Aspergillus spp.), in stark contrast to C. albicans, even feeds on bismuth subsalicylate (Pepto Bismol) / subcitrate to grow its biomass!I appreciate your hint to oral ibrexafungerp (SCY-078)! A totally new class of antifungal I hadn't even read before which directly inhibits fungal 1,3-beta-D-glucan. It sounds highly promising also for systemic action. US licencing only for vulvovaginal candidosis so far. Fosmanogepix is also another first-in-class with orphan drug status.
Both are strongly lipophilic, however. Haven't read much further into them yet.I have two more days of flucytosine ahead of me, then totalling 24 days.
Together with EGCG appears to be the best combination for liver and biliary tract access.
I'm still affected by the weak and woozy head but less consciously aware of it. Maybe I grew accustomed, maybe it lessened a little bit. It did not increase over time nor with the FCy dose increase, and the initially associated rise in depression faded. Overall making me think it's due to antifungal effects at work beyond a perhaps baseline toxicity.Artichoke leaf extract hugely increases bile synthesis and release any may be a long-term way option along with intraluminal antifungals. However, ALE also hugely increases MMC, i.e. transit speed. Just as coffee, or nicotine, or cholinergics, or anything prometabolic like sunshine, B2, B1, B6, B5, B3, Mg, K, betaine/TMG, menaquinone do.
This is hugely confounding. I'm likely to have some sort of profound autonomous nervous system damage with dumping syndrome probably as a result of multiple severe GI infections. I.e. the nerve endings and regulation of my intestines are shot and fried. Unable to heal by themselves. The harm is comparable to the neuropathy in late-stage diabetics. It does not only occur after GI surgeries as Mickey Mouse clinicians make-belief.Interesting that cannabis (pain medication) is mentioned as an exacerbating trigger.
SST/octreotide may help but I cannot get hold of that.
BPC-157 may actually cure:Stable Gastric Pentadecapeptide BPC 157 May Recover Brain-Gut Axis and Gut-Brain Axis Function, 2023
-
@CrumblingCookie bpc actually works really well for intestinal issues. you dont need the arginate salt either, the commonly available acetate one is fine. the marketing on the former makes it sound otherwise. i actually looked into buying the patent for the arg form but it became clear they were just trying to offload the intellectual property because they realized there isnt really a market incentive for it
if you find ibrexafungerp somewhere id like to know. it’s like $150 a pill from GSK with a doctor’s prescription and without insurance coverage. the company that invented it actually probably sold it for too cheap imo. by what it sounds like it can probably replace fluconazole as an otc single pill form that are sold for women’s yeast infections at various drug stores.
-
UDCA and TUDCA appear to be rather neutral towards fungi from what I can find.
I thought TUDCA was helpful on the basis of it being a secondary bile acid. But I also didn't find studies on that...
I've been taking TUDCA for about 10 days. And my body seems to get used to it. In the beginning it lead to loss of water retention, fuller muscles, better liver function and even a bile dump. Now it doesn't seem to do much anymore. Not sure why. But I often have the experience that I develope tolerance to things rather quickly.
I'had looked into therapeutic DCA use as well but it's also strongly cytotoxic to human cells. Or perhaps I'm not remembering correctly and endogenous DCA abundance is always being mixed up with a concurrent abundance of the more harmful LCA.
Yes I think it's also cancer inducing. And hard to find. Not even sure how you got the UDCA. Do you think there's any reason to take UDCA if I've tried TUDCA?
gentian and taraxacum are the basic cholagogics I believe tincture of gold coin grass aka Lysimachia aka Jin Qian Cao or glechoma hederacea was a profoundly effective addition back then, too.
Interesting I will check those out.
Have you guys tried serrapeptase or allicin?
The Biofilm buster + anti fungal protocols are quite popular on reddit and such forums. I do notice anti fungal effects from nattokinase. -
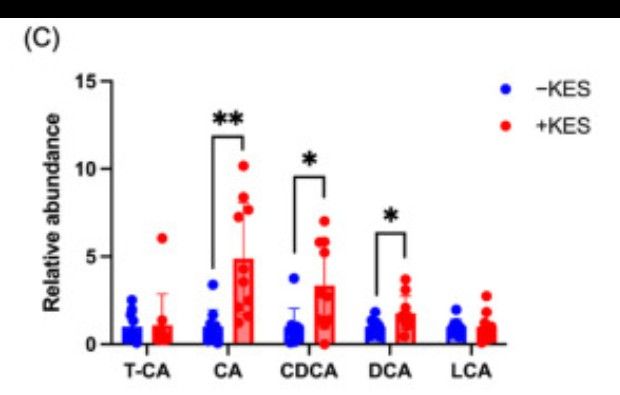
Kestose could be an interesting candidate. It increases deconjugated bile acids and increases bacteria that deconjugate bile acids.
Also increases 5aR in another study."...the levels of deconjugated bile acids, which are involved in the regulation of lipid synthesis, were increased. Furthermore, the 1-kestose intake altered the gut microbiota in the cecum, leading to an increase in the abundance of specific bacteria, such as Bifidobacterium, which are involved in the deconjugation of conjugated bile acids."
It strongly increases Cholic acid and other bile acids .
-
Have you guys tried serrapeptase or allicin?
The Biofilm buster + anti fungal protocols are quite popular on reddit and such forums. I do notice anti fungal effects from nattokinase.ive tried serrapeptidase and of itseld it is an effective biofilm buster, both for external (from mouth to anus) and internal (vasculature and lymphatics). I have to find a dosage that would throttle the rate at which biofilm, as well as plaque, is lysed. And I have to cycle its use as well. I have to do a cbc weekly, to be able to see my wbc, as the contents held back by biofilm from lysed plaque as well as lymphatic biofilm, lead to a strong innate immune response, as seen by my wbc going very high (12 is the highest, compared to a reference range high of 9), but I think it will get higher if I just kept taking serrapeptidase, especially the high dose versions). I'm told that the high release rate of pathogens would lead to high levels in the blood, which would be detected in a cbc, and that is usually called bacteremia, though that is just a catch-all, as what's released may also nit just be bacteria but fungi, and virus(if I believe in their existence), as well as toxins, especially heavy metals). I was afraid it would trigger sepsis, but I am told that it won't happen, but even the bacteremia at veryhigh levels would have a very high inflammatory effect. My system could be overwhelmed still, and the last thing I want is to go to the ER not walking in but being brought in by an ambulance.
n.b. When I said I'm being told, it is my Deepseek AI, which I find gives me unpeaty answers initially but when AI challenge it would come to agree with many. Something I see positively than talking to most humans, especially doctors.
Since we are talking antifungals also, I have so far avoided pharma anti-fungals, having used essential oils that are esters, and put different essential oil esters together so they can have multiple pathways of action, more than what just one essential oil would have, given that each essential oil Ester brings its own combo of esters into the table. Esters are known for their antifungal properties. I make my own suppositories that have these essential oils in a carrier oil (coco butter, mct, vco etc]. Lately I have shown a preference for vco as it also contains a lot of lauric acid, which is anti-fungal. I like suppositories because it bypasses the liver first-pass.
Maybe serrapeptidase plus essential oils is enough, but it is highly dependent on my shoice of essential oils, and on this it is very hit or miss in its nature of being trial and error. But It is still effective though if I think whether it is 100% it may be with enough use over a period of time. As to use it as a stack with serrapeptidase could give it added potency.
Still, I have found it ineffective against a nagging knee pain on both knees, felt when I rise up from sitting, and when I walk up the stairs. That led me to taking borax of 3 x 30mg daily, which amounts to 10mg of boron daily. The cause of that knee pain is said to be fungal, and borax is an effective anti-fungal. I only came to use it last week and it actually lowered my eosinophils in my wbc differentials in my cbc. I am highly certain the drop in my eosinophils from 4.5 percent to 3 percent came from using it, as that was the only antifungal treatment I took last week. But last week I was taking 1 x 300mg of borax daily, which was an overdose. I corrected the dosage and am back to a sage daily dosage of 90mg (3 x 30mg). This morning, waking up, I felt less creaky joints, but it's too early to say but it likely would work at least for the kneess, as this was what Rex Newnham, the Australian doctor, sold his boron supplements for before the supplements were banned.
Next week, I should start a new protocol that had been sitting on the sidelines for 2 weeks because I felt it was lacking something and my mind was off gallivanting not necessarily focused but on a break hoping I would get a pleasant form of collateral damage. It did when I chanced upon a post on Threads about boron as an effective fungicide for industrial use. It made me come back full circle on using boron, which I had not developed enough respect for. Had taken it before, but in a way that says "what the heck, nothing ro lose."
-
Interesting thanks for sharing. which essential oils do you find to be most effective ?
-
@sunsunsun Thanks. How much and for how long had you been taking BPC orally? And what did it do for you?
I've started pinning 500µg pd yesterday. If it works as great as I desperately hope it will I'll be drinking it, gargling it, snorting it, dripping it in my eyes and ears and rubbing my face with it.@mauritio Serrapeptase is powerful. Gave me painful colon cramps even stronger than from pancreatic enzymes, which I assume fits in dumping syndrome as it reached lower GI parts it should never have without prior absorption.
But against fungi in particular I don't know. There are a few enzyme products which also contain (hemi)cellulases which I'd rather choose. Cellulases are the next best thing to actual chitinases to break down that respective part of fungal cell walls and biofilm.
@mauritio The allicin supplements seem like a well laid-out scam to me. The high prices and the tiny allicin contents are ridiculous. That's why chose fresh garlic. It's crucial to wait at least 10mins after crushing it so that alliinase can convert alliin to allicin.
@mauritio I reckon you're fine with TUDCA. I chose UDCA because I (A) reacted badly to extra taurine, (B) it's the medically used form, (C) it's cheaper.
I got it from my favorite dear courtly purveyor of fine powders from the lands of plenty far far east.
Just a thought I got: To keep an eye on repleted choline when you're staying keen on bile expulsion.
@Mauritio Kestose sounds more like an alternative to fat binders if the goal is to lose body fat through constant steatarrhea and bile acid loss. To not be bothered by these changes I reckon one's stool must be quite good already or even on the dry, constipated side. -
@CrumblingCookie once in awhile if I forgot not to lie down immediately after taking aspirin (can cause heartburn) or take aspirin on an empty stomach and it feels irritating I will take 250mcg-500mcg bpc and it cures it. a reconstituted vial lasts months in the fridge in the dark.
are you going to take florastor when you are done the anti fungal protocol?
-
@sunsunsun starting chemotherapy for acne
-
@sunsunsun Mhh... I was going to say no but now you've made me ponder whether it'd be good for a stretched-out transition of suppressing Candida species recolonization. Or whether its effects would be as bad on physiologic restoration as taking bacterial probiotics after antibiotic treatment...
It'd probably be good though to spend time along healthy forests and meadows in order to pick up a symbiotic mycobiome, I imagine. Perhaps to do both.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login