DHT as an alternative for TRT
-
Have you tried pct? To my understanding there are bodybuilders that blast T for a decade and then get off it using clomid or other such drugs, and their T levels are only slightly affected. This may be useful for getting to a reasonable baseline for endogenous production for t.
-
-
@jamezb46 Thanks
-
This post is deleted! -
@ooopilled said in DHT as an alternative for TRT:
I wonder if it’s possible that just pregnenelone, thyroid, and dhea could get me from 15ng/dL to a good healthy T level ?
thoughts? @jamezb46
-
Well, I think we need to keep in mind that Ray was probably talking about oral or transdermal testosterone, not injectable.
But, ya you could also try the idea labs product Pansterone orally or transdermally. People have reported it boosted their T levels.
-
@jamezb46 Also if im not mistaken the T boost from pansterone would be most likely from the DHEA rather than the pregnenolone, while pregnenolone seems to metabolize into progesterone more than anything? Ive also heard from Hans that DHEA boosts T in a very dose dependent matter (i.e. 50mg can give you a 25-50ng/dl boost, 100mg can give you a 100ng/dl boost, 200mg can give you a 200ng/dl boost. etc) but iirc those high doses would be very estrogenic and Ray Peat recommended doses under 15mg.
-
@jamezb46 Do you think proviron alone could act as “testosterone replacement” in my case or would I still need to pair it with standard TRT since my baseline levels are so low?
-
@ooopilled Lets say I did 25mg proviron + 15mg pansterone. Could this be comparable to a standard TRT dose of 150-250mg test or would it not compare?
-
@ooopilled It likely wouldn't compare, according to this study:
https://link.springer.com/article/10.1007/BF03348281
A group was given 120mg of testosterone undecanoate daily orally. Note that oral testosterone undecanoate, has a half life of a few hours, due to first pass metabolism. It does not build up in the system, and has a much shorter half life than proviron (12-13 hours),
Another group was given 150mg of mesterolone (Proviron) daily, and the effects were compared.TU is the testosterone undecanoate group & mesterolone is the Proviron group
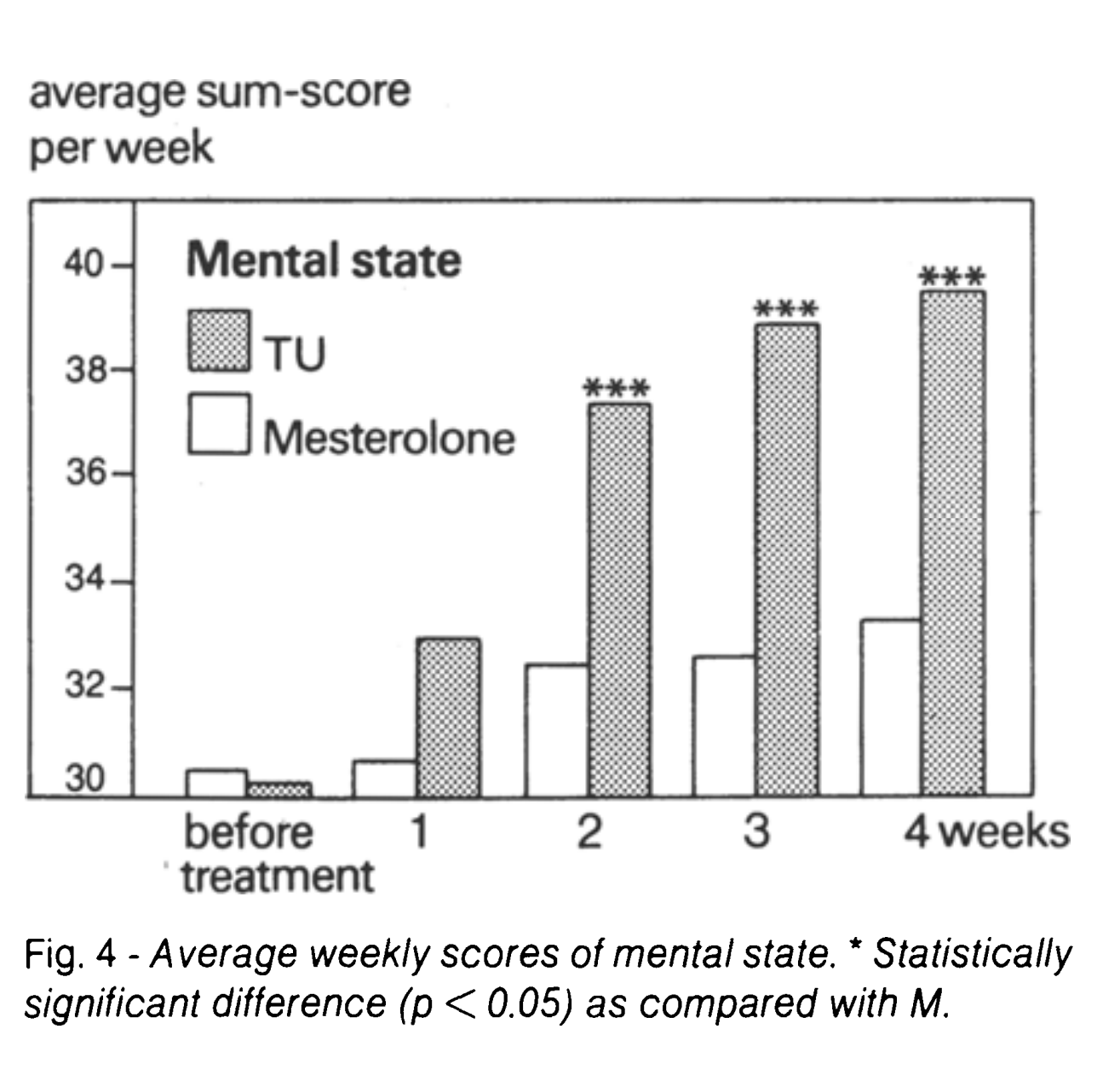
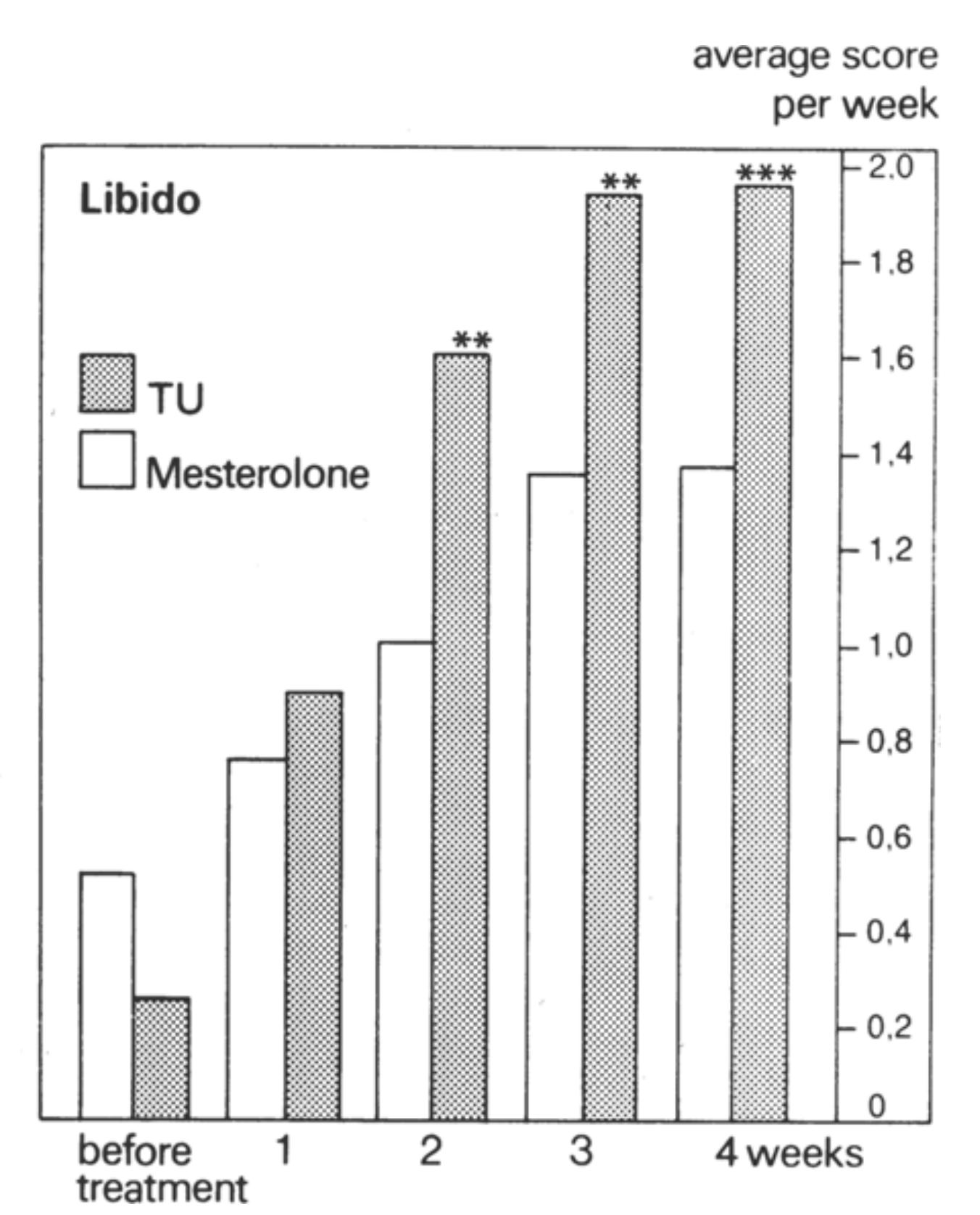
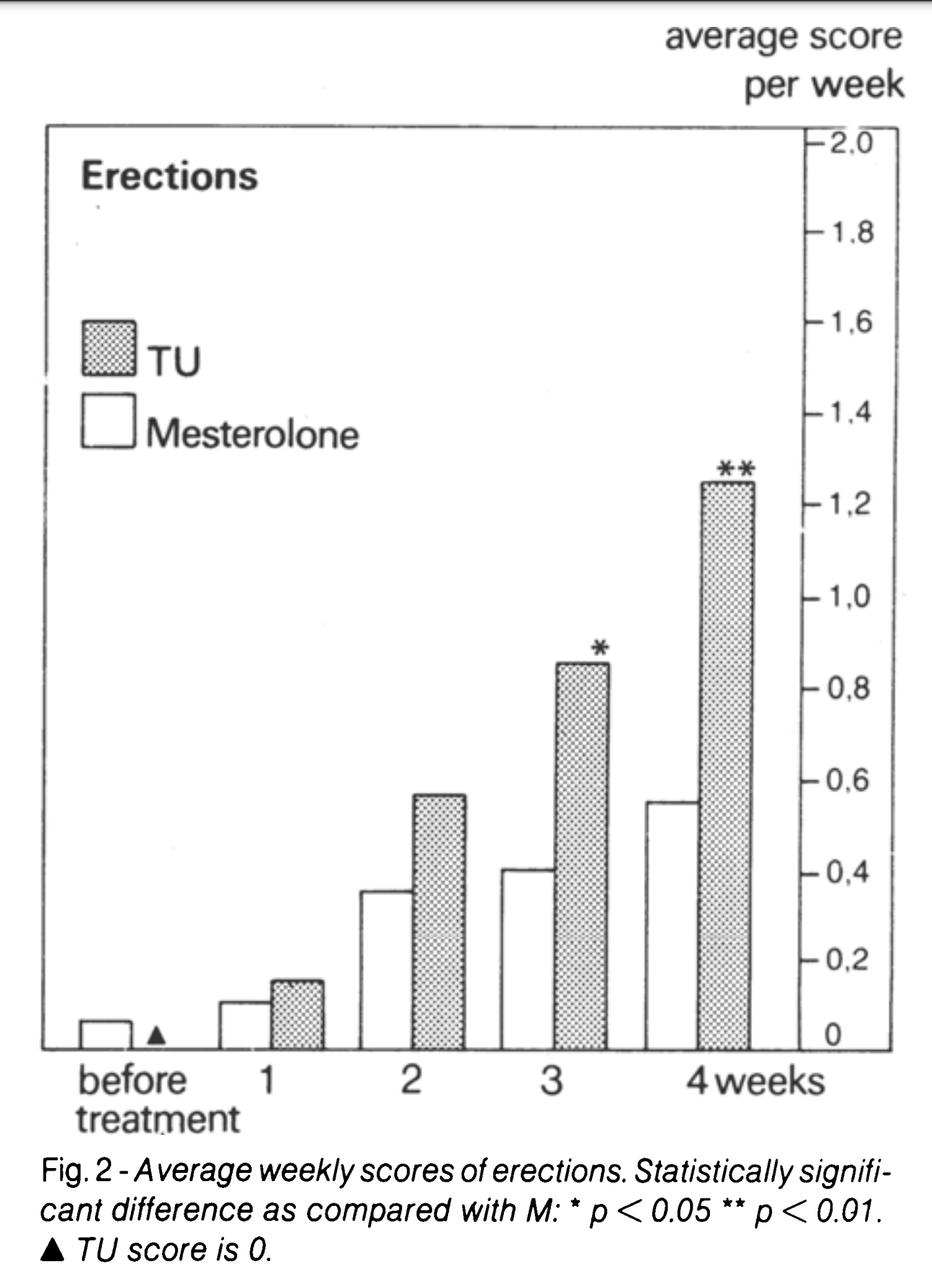
"The effects seen for TU on these variables are much better than those observed for M. The low activity 01 M found in this study is in agreement with observations by other authors (10 - 12) and by ourselves (Franchi unpublished data). In view 01 this low activity we decided to use a considerably higher daily dose of M than that recommended. "
Proviron does seem to bring strong mental benefits; a study showed it was as effective as SSRIs in treating depression. However, this is likely due to neurosteroid metabolites, and not due to Proviron being a decent androgen. In the end, Proviron does not shut down the HPG axis, and this is a clear sign that it does not considerably agonise the androgen receptor in humans
Furthermore, as James pointed out, Proviron is only available as a pharmaceutical in the middle east, such as Omar and Kuwait. Any "Proviron" currently sold by vendors, are guaranteed to be counterfeit, as it is not even produced in Turkey or anyother country anymore, and it is a very rare medication to be prescribed. This is verified by personal experience as well, as the Proviron I received from Turkey, were revealed to be counterfeit when I scanned their QR code on the Turkish medicine verification app.
Therefore, proviron has the disadvantage of only being available from underground labs, if you want a drug you can trust is real, use TRT as you can get that prescribed in the US.
-
@alfredoolivas apparently dbol doesnt shut down lh fsh to a high degree on a cycle yet it is quite anabolic so what say you then
-
@sushi_is_cringe I doubt that. Which study and what doses were used? The doses used medically tend to be quite low. With Mesterolone / Proviron, the medical community actually noticed it's lack of effectiveness, and that's why studies were performed with doses mesterolone, up to 150mg a day, as they were trying to push it's limits. Even with these 100mg+ doses, it seemed to be non-supressive in most people. With the regular 25-50mg doses? Unsuppresive for all patients.
-
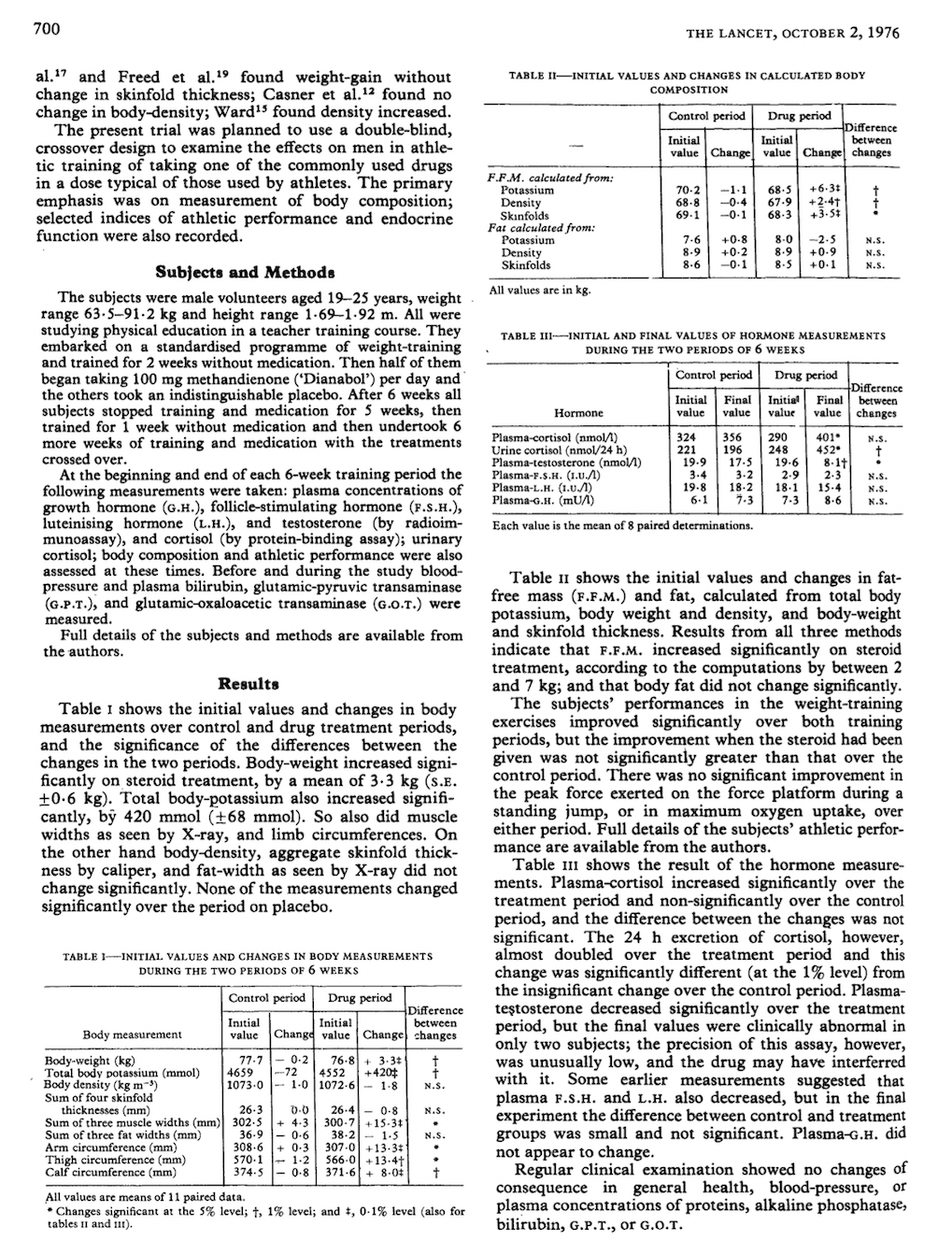
I have the study.
"Anabolic" effects of methandienone in men undergoing athletic training
G.R Hervey October 1976, Published in The Lancet
100 mg Dbol per diem for 6 weeks. LH, FSH had no statistically significant decline, but testosterone fell by about half. That suggests that there is primary transient hypogonadism because there is enough LH, FSH in the blood but the testicles are not producing enough testosterone. That leads me to think that there is some negative feedback directly in the testicles.
It could also be that there is excessive conversion to estrogen, but I think the testicles are also being inhibited.
-
@jamezb46 Very interesting. Yes, the testicles will reduce their expression of crucial steroidogenic enzymes, in response to more androgen agonism in the testicles.
https://sci-hub.se/10.1111/j.1749-6632.1984.tb38367.x

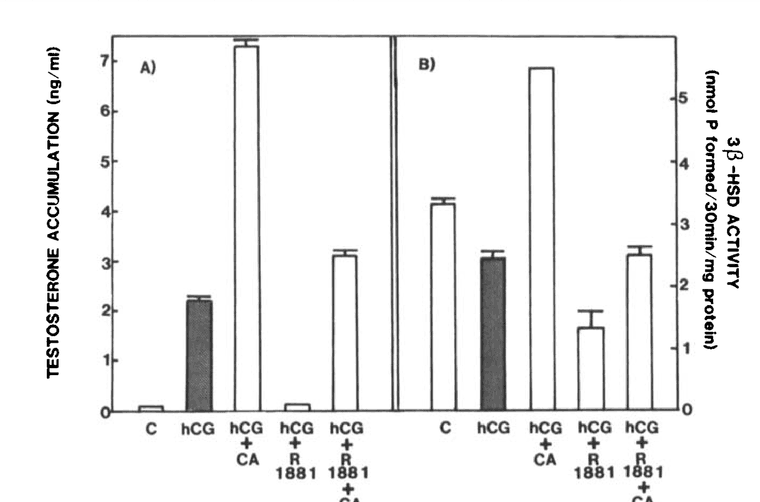
As seen on the graph, R1881 / Methyltrenbolone, was able to reduce hCG stimulated expression of intratesticular 3-beta HSD levels.Estradiol also does the same
https://pubmed.ncbi.nlm.nih.gov/3862577/@jamezb46 said in DHT as an alternative for TRT:
@alfredoolivas
It could also be that there is excessive conversion to estrogen, but I think the testicles are also being inhibited.Generally, a minuscule amount of androgens are converted into estrogen. Testosterone is roughly 200–1,000 times higher than estradiol in concentration.
That is why androgens are measured in ng/dl, whereas estrogen is measured in pg/dl.
So it's impossible for testosterone to be significantly lowered, due to aromatase "stealing it" and turning it into estrogen. Estrogen will only lower testosterone by inhibiting LH and lowering steroidogenic enzymes. And it does so very well
-
@alfredoolivas
https://haidut.me/?p=1317
"Normal men produce ~45 mcg of estradiol each day, a sixth of which is secreted by the testes and the remainder of which is derived from the extraglandular aromatization of circulating androgens"Only 45mcg of estradiol is made daily from the 20-25mg (my estimation of DHEA, testosterone, androstenedione levels?) pool of aromatasable androgens, so yeah, the aromatase enzyme isn't directly lowering androgen levels by stealing androgens, even if it is extremely elevated @jamezb46
-
Yes, but its downstream effects are inhibiting T production.
I wonder if Ray’s suggestion to use Pregnenalone to safeguard the gonads would work to preserve their steroidogenic potential even in the presence of high levels of circulating androgens?
And if that did work, perhaps using topical Pregnenalone, k2, and caffeine on the scrotal skin would be even more effective.
-
@jamezb46 Are you referencing this study?
Pregnenolone (P5) fully prevents testicular atrophy due to steroid (ab)use or high estrogen
According to Haidut's calculations, this study has shown that pregnenolone used in doses of 10x -15x that of testosterone, will fully prevent gonadal atrophy, from testosterone and estradiol.
Not sure if the studies he referenced showed the levels of intratesticular steroids after the pregnenolone, but maybe one can assume that pregnenolone improved intra-testicular levels of androgens.
However, he also referenced this study showing that testosterone can actually inhibit gonadal atrophy, and is gonadotropic.
“…It will be seen that at low dosage levels delta-5-pregnenolone is even more gonadotropic than testosterone, methyl testosterone, androstenediol or dehydro-iso-androsterone, while at the 10 mg. dosage level delta-5-pregnenolone is less effective than the above compounds. ....small doses of testosterone cause a testis atrophy which is not seen at high dose levels (1 1). This fact could best be explained by the assumption that comparatively low doses of testoids inhibit the gonadotropic hormone secretion of the pituitary and thus cause a secondary testis involution which, in the case of high doses, is over-compensated by the direct testis-stimulating effect of these compounds."
"As it has recently been shown that the testis atrophy caused by estradiol can be inhibited by testosterone and progesterone[2,3]"
This makes perfect sense given testosterones (and all other androgens) anti-estrogenic effect
This actually explains my experience with testosterone very well; I have been currently, running 2100mg of test enanthate a week, for the past 9 months, and have not seen a too significant reduction in semen volume.
-
@alfredoolivas dude your nuts arent shrunken ?
at 140mg test cyp a week i got no noticeable nut shrinkage but also no noticeable positive effect
at 350mg or maybe it was 500mg i cant remember i got definite nut shrinkage and major side effects. i was also not peaty at all at the time . i imagine i could take that dose and be mostly fine now
how tf are u running 2100mg tho lol
-
so if i take 34mg (a fibonacci number) of dbol per day split throughoutbthe day (best way to take it) orally and 5mg of dht transdermal i should also take like 400mg of pregnenolone a day? seems a lot maybe just 50-100mg in tocopherol for higher absorption would be good
-
@alfredoolivas pls post ur physique . some of the stuff you say sounds retardo but at the same time i dont intend to dismiss it without an actual reason for prejudice. the answer lies within an image of ur physique
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login