Inosine directly binds and blocks the endotoxin/LPS receptor (TLR4)
-
Inosine is an endogenous purine and a breakdown product of ATP. Elevated inosine levels are observed in stress and many chronic conditions, and medicine has so far viewed those changes in inosine levels as simply a natural metabolic cascade, with few direct effects of its own. Inosine can also serve as a precursor to ATP through the inosine->IMP->AMP->ADP->ATP salvage pathway and older studies in the former Soviet block counties demonstrated that inosine supplementation has a number of beneficial effects on tissues, immunity, mood, etc. In fact, inosine was used back in the day as kind of over-the-counter (OTC) doping drug by many athletes from those countries as it was believed it would lower inflammation and boost muscle mass/strength. However, subsequent studies in the West apparently failed to replicate the ergogenic effects of inosine and the substance has thus been declared as being little more than a metabolic “waste”, especially given its ability to further metabolize into uric acid and thus contribute to gout. I will soon do a separate post on inosine and its ergogenic effects, but it appears that the study below validates at least the claims for anti-inflammatory effects of inosine. Namely, the study found that in physiological concentrations inosine directly binds to and deactivates the TLR4 receptor, through which endotoxin exerts most of its systemic inflammatory effects. This suggests that the elevations of inosine during stress/disease conditions is likely not just pathological but adaptve as a way to lower systemic inflammation. This makes inosine a true TLR 4 antagonist, and a substance of particular interest given how few such OTC substances are known to medicine and the role of endotoxin/LPS/TLR4 in virtually all chronic conditions. And last but not least, the study below provides a plausible mechanism of action for the known protective effects of inosine in many viral conditions, which appear to exert their damage mostly through systemic inflammation, usually driven by endotoxin/LPS.
https://doi.org/10.1016/j.phymed.2025.156854
“…Treatment with inosine led to significantly attenuated lung injury, improved pulmonary function, and reduced levels of IL-1β, IL-6, IL-18 and TNF-α. Specifically, inosine promoted M1-to-M2 macrophage polarization, thereby enhancing anti-inflammatory responses. Clodronate liposome depletion led to degradation of protective effects of inosine, indicating a key role of macrophages. Metabolomics analysis revealed that treatment with inosine restored glycolysis, lipid metabolism, and amino acid homeostasis, while transcriptomics analysis showed downregulation of TLR4/NF-κB, PI3K-Akt, and NOD-like receptor pathways, with upregulation of anti-inflammatory genes**.** In vitro tests indicated that treatment with inosine led to decreased apoptosis rate of LPS-induced 16HBE cells, decreased levels of inflammatory cytokines, and inhibited TLR4 activation, and such effects were enhanced by TLR4 inhibitor TAK-242. SPR analysis confirmed that inosine can inhibit signaling of TLR4 via direct binding. Inosine shows protective effects against ALI as it may regulate TLR4 signaling to modulate macrophage polarization, metabolic homeostasis, and inflammatory responses. This study comprehensively integrate multi-omics analysis and functional assays to reveal the direct interaction between inosine and TLR4 for the first time, and provides insights into its anti-inflammatory and immunoregulatory mechanisms.”
-
People considering inosine supplementation for the above will also want to intentionally activate mTORC1/2 and inhibit AMPK. It's daft. Yet anabolic as long as the serious negatives don't catch up with you.
-
Inosine also converts to uric acid quite readily which is why it was abandoned as an ergogenic in the 80's
-
Its abandonment due to uric acid was most likely part of trickery science: the stuff controllers and such set up to create sleight of hand. In the old forum around I think it was 2015 or 2016, I had mentioned I suspected gout to be not of a uric acid problem but of a metabolic one. One induced by pufa consumption. Fast forward to 2021, and Wie-Zheng Zhang established in "Why Does Hyperuricemia Not Necessarily Induce Gout" that inflammation was the true driver. Now I think even some of these good researchers still have a ways to go to form a whole-picture idea, but researchers and studies like this are a step in the right direction. Rather than the mechanical "uric acid goes up, and gout happens," it is now being understood gout is an afflicted immune problem (take note I do NOT say autoimmune; that idea is utter crap), based on systemic inflammation; even calling it a type of arthritis. Uric acid being most likely a compensatory and defensive reaction. I even said in that old thread on the old forum uric acid is hijacked. These shallow, mechanistic correlations are made to say good things are bad. SUCH as inosine. The immediate correlation to increased uric acid also equates to "inosine bad."
Incidentally, one of the most important pieces of evidence is that only about 36% of gout patients have high levels of uric acid.
-
The only two folks I’ve know that have serious gout are heavy drinkers. And old. And pretty sharp minds too. Like excitatory Adrenalin or something. No science here just anecdotal bs so I can fallow others thoughts on this thread.
Cheers -
You take inosine WITH a xanthine oxidoreductase inhibitor such as apigenin —you raise ATP and raise your metabolic rate…there are numerous clinical trials with inosine + feboxostat but there is no need for a Big Pharma drug to do this yourself.
-
@bio3nergetic said in Inosine directly binds and blocks the endotoxin/LPS receptor (TLR4):
most likely part of trickery science: the stuff controllers and such set up to create sleight of hand
Those pesky evil scientists.

Now I think even some of these good researchers still have a ways to go to form a whole-picture idea, but researchers and studies like this are a step in the right direction.
It could be viewed as a disorder of fluid turnover. If there's an issue with exchange over the synovial membrane or those ahead of it, that could explain discrepancies in uricemia markers.
-
@dapose This is a good insight into the inflammation variable as what heavy drinkers exhibit. When I used do nutritional consulting, a couple of clients had gout that cleared up with diet change, namely the pufa exposure.
-
Fascinating. Have you experimented with it yourself or know of people who have dialed in the dosages?
-
@jamezb46 said in Inosine directly binds and blocks the endotoxin/LPS receptor (TLR4):
Fascinating. Have you experimented with it yourself or know of people who have dialed in the dosages?
Yes. 500mg - 1000mg twice a day of inosine. I’ve used 100mg or so of apigenin. You can also use a single drop of Eugenol instead.
Try it. It works very well. I’m doing a different experiment now, but I’ll come back to this soon.
-
Thanks so much for responding. When you mention increased ATP and increased metabolic rate what kind of phenomenological effects does that manifest as? Increased temp? pulse? more sharp cognition? less fatigue? less lactic acid feeling in muscles?
-
@jamezb46 yes all that. Just remarkable clarity. There are a number of clinical trials for this approach. It can probably reverse autism.
-
Inosine arrives today, and I already have clove bud oil. I’m going to trial 500mg Inosine and one drop of clove bud oil, (in a gelatin cap) once a day for two weeks.
I rely predominantly on charcoal for TLR4 management, (though that comes with its own disadvantages). I’ve tried D3, Bs, antihistamines, and many of the other so called TLR4 antagonists, but nothing works for me personally like charcoal. My goal is to find something other than charcoal that I can reach for with equal effectiveness.
-
@evan-hinkle incidentally, just 500mg or 1000mg of charcoal every few days makes a dramatic impact without any of the negatives of larger amounts.
-
@Ecstatic_Hamster this is actually what I do now, but the day after my dose of charcoal typically slows my transit time, and for whatever reason I just can’t feel optimal without daily consistency, (I assume due to years of unchecked, and totally undiagnosed low-grade sepsis).
My hope is to be able to antagonize TLR4 while maintaining fast, complete, and regular transit. Otherwise forward progress for me tends to be a bit like sprinting on a treadmill, (I don’t move forward, just keep-up so to speak).
-
@evan-hinkle said in Inosine directly binds and blocks the endotoxin/LPS receptor (TLR4):
My hope is to be able to antagonize TLR4
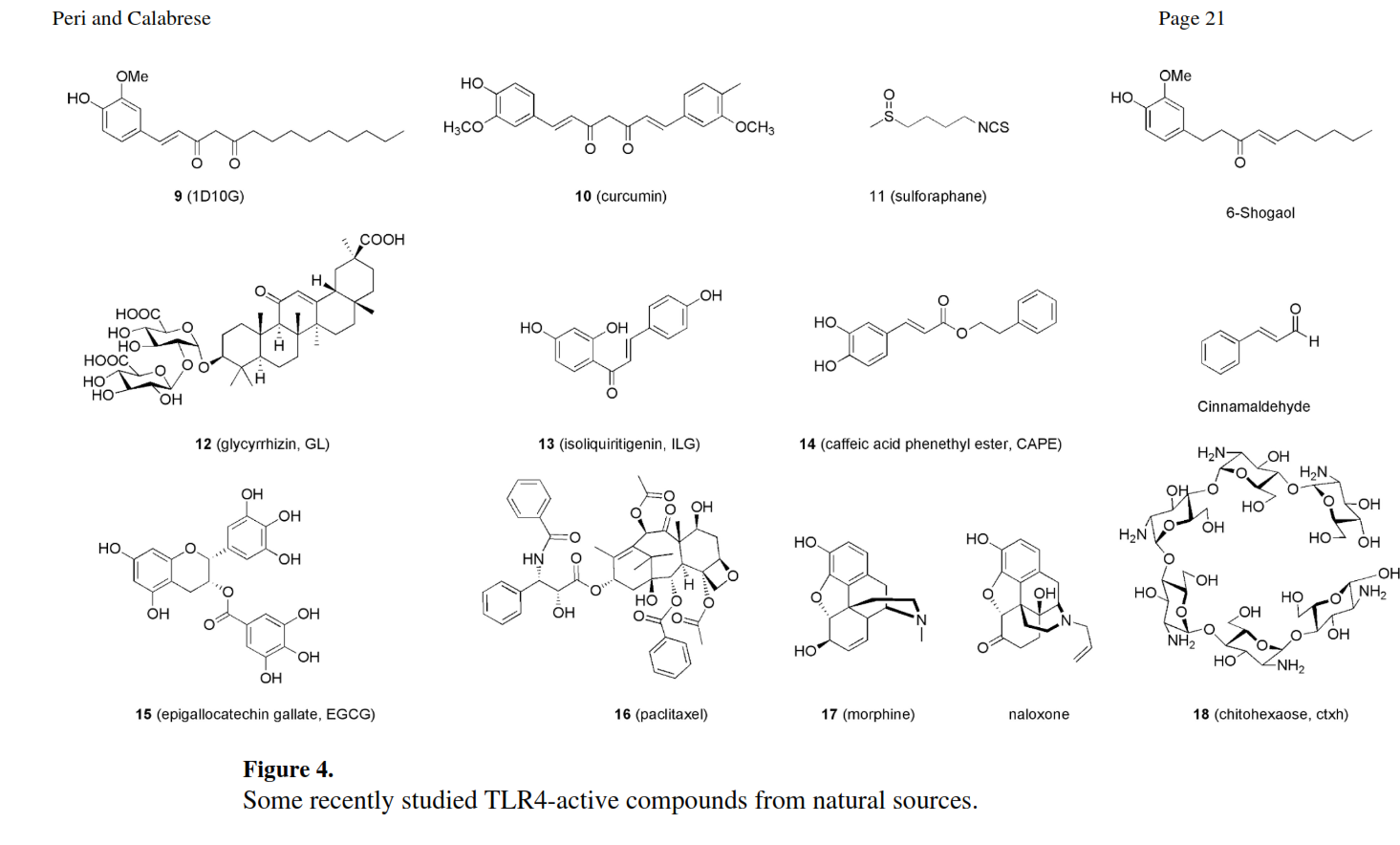
Some natural TLR4 antagonist that you might consider sprinkling into your diet include:
Dried ginger is a savory source of 6-Shogaol.
-
@evan-hinkle said in Inosine directly binds and blocks the endotoxin/LPS receptor (TLR4):
@Ecstatic_Hamster this is actually what I do now, but the day after my dose of charcoal typically slows my transit time, and for whatever reason I just can’t feel optimal without daily consistency, (I assume due to years of unchecked, and totally undiagnosed low-grade sepsis).
My hope is to be able to antagonize TLR4 while maintaining fast, complete, and regular transit. Otherwise forward progress for me tends to be a bit like sprinting on a treadmill, (I don’t move forward, just keep-up so to speak).
doing the honey diet with intermittent reset days, bowel movements are loose enough and fast enough so the charcoal is absolutely beneficial to me, and not a problem at all, quite the opposite.
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login