B-complex and or Multi recommendation?
-
@albion said in B-complex and or Multi recommendation?:
Would you recommend someone trying to diagnose if they need more Cysteine to take NAC? If yes, just as a diagnostic tool or ok as a regular/intermittent supplement?
Mind the combination of NAC with B3, if high dose, at a prolonged use.
*) When Niacin(or vitamin B3) and NAC (N-acetyl cysteine) are combined, especially under specific pH and concentration conditions, a chemical reaction may occur that forms pyrazinic acid (pyrazine).
Most sources specify that no interaction has been found between NAC and niacinamide (or nicotinamide). This is incorrect when there is prolonged concomitant use with a high dosage of NAC.
The toxic effects of pyrazinic acid may include cellular damage and oxidative stress, which is of particular concern for people with predispositions to oxidative stress-related diseases.Sources and References
- Hepatotoxicity related to anti-tuberculosis drugs: mechanisms and management
https://doi.org/10.1016/j.jceh.2012.12.001 2013.
The toxicity of pyrazinamide is both dose dependent with a higher dose at 40–50 mg/kg, with NAC combination. (2 800 to 3 500 mg NAC for 70 Kg/weight, or +/ 170 Lb). - Unproven (questionable) cancer therapies.
ML Brigden - Western Journal of Medicine, 1995 - ncbi.nlm.nih.gov
Mega-doses of vitamin B3 (niacin) have liver toxicity and have produced acid peptic disease,
myocardial infarct, gouty arthritis, glucose intolerance, hyperkeratosis, and skin rashes."
- Hepatotoxicity related to anti-tuberculosis drugs: mechanisms and management
-
-
@GRay said in B-complex and or Multi recommendation?:
I just took a quick look at it, there is citric acid in it.
Can you tell me roughly the danger of citric acid? Is there a Peat article on it?
-
@Corngold I didn't really retain much info on Citric Acid, I heard Georgi talking about it many times in a negative way as cancer promoter, perhaps Ray Peat has some article or interview about it.
-
@wester130 I know this company. It looks good, I like it since it doesn't have B12 in it. However it doesn't have the B5 in it though, which I think it can be helpful for adrenal hormone production.
-
Since I'm ingesting allot of B12 from food, beside the 8oz of liver I have weekly I also eat 1lb of beef heart as well, plus 3 eggs daily, do you think adding more B12 with a B-complex once or twice weekly can be an issue?
it seems like the products I like they also contain the B12, beside Energin and the B-complex from Forefront
-
@GRay said in B-complex and or Multi recommendation?:
I heard Georgi talking about it many times in a negative way as cancer promoter
Not at this dose, in a supplement, as an antioxidant (citric acid).
The dual role of citrate in cancer
Excerpt
In this context, targeting citrate and citrate-related metabolism [[6], [7], [8]] may appear to be a novel and hopeful option. Citrate is an intermediate of the tricarboxylic acid (TCA) cycle (also known as Krebs cycle). In the cytosol, it is cleaved by ATP-citrate lyase (ACLY) into oxalacetate (OAA) and acetyl-CoA. The latter is the primary substrate for fatty acid (FA) synthesis (FAS) or protein acetylation (either in the cytosol or in the nucleus for epigenetic modifications). Increased de novo FAS is one of the hallmarks of cancer cells, as well as an increase in aerobic glycolysis, the so-called Warburg effect [9]. Therefore, an adequate citrate supply is crucial to sustain cancer cells growth. However, citrate is also a Ca2+ and Mg2+ chelator, as well as a potent inhibitor of phosphofructokinase-1 (PFK1), the key regulatory enzyme of glycolysis [10], and also of phosphofructokinase-2 (PFK2) [11], which produces fructose-2,6-bisphosphate (F-2,6-BP), the main potent activator of PFK1 [12]. Consequently, proliferative cancer cells need to strictly control their intracellular citrate level to keep their metabolism balanced. Indeed, while a low level of citrate could impair cancer cell growth due to decreased FAS, an excessive level may have detrimental effects on glycolysis, ATP production and cell survival [13,14]. Therefore, such a need for a strict control of intracellular citrate level by cancer cells may offer two strategies potentially valid for cancer treatment, i.e., (1) reducing intracellular citrate levels (for example by inhibiting citrate uptake) and (2) flooding cells with excessive citrate to arrest glycolysis.
https://doi.org/10.1016/j.bbcan.2023.188987
Science Direct 2023. Philippe Icard et al. -
@albion said in B-complex and or Multi recommendation?:
@CrumblingCookie Would you recommend someone trying to diagnose if they need more Cysteine to take NAC? If yes, just as a diagnostic tool or ok as a regular/intermittent supplement?
IMO both is possible. NAC is much much less excitatory than free cysteine and really good as long as there's no diarrhea from taking it. In the latter case it's better to work up with sulfate. It's difficult to forecast the full circle of interdependencies which depends on individual overall health.
For regular or continuous intermittent use I'd blend the NAC 1:1 with glycine and add a basis of 100mcg molybdenum per day. Lots of vegan protein powders are especially poor in cysteine (and total sulfur amino acids) so adding NAC to them can make them feel much more wholesome and nutritious imo. -
If I'm understanding correctly, NAC is actually beneficial as some studies show, totally different from Cysteine?
I supplemented with NAC for years, but put it aside since in the Peat world.
-
@GRay Yes. In the notoriously and rightly bashed context of free cysteine, NAC is very different.
With NAC:
The combination of slow uptake and a deacetylation step that is not extremely efficient is expected to limit the intracellular delivery of Cys.
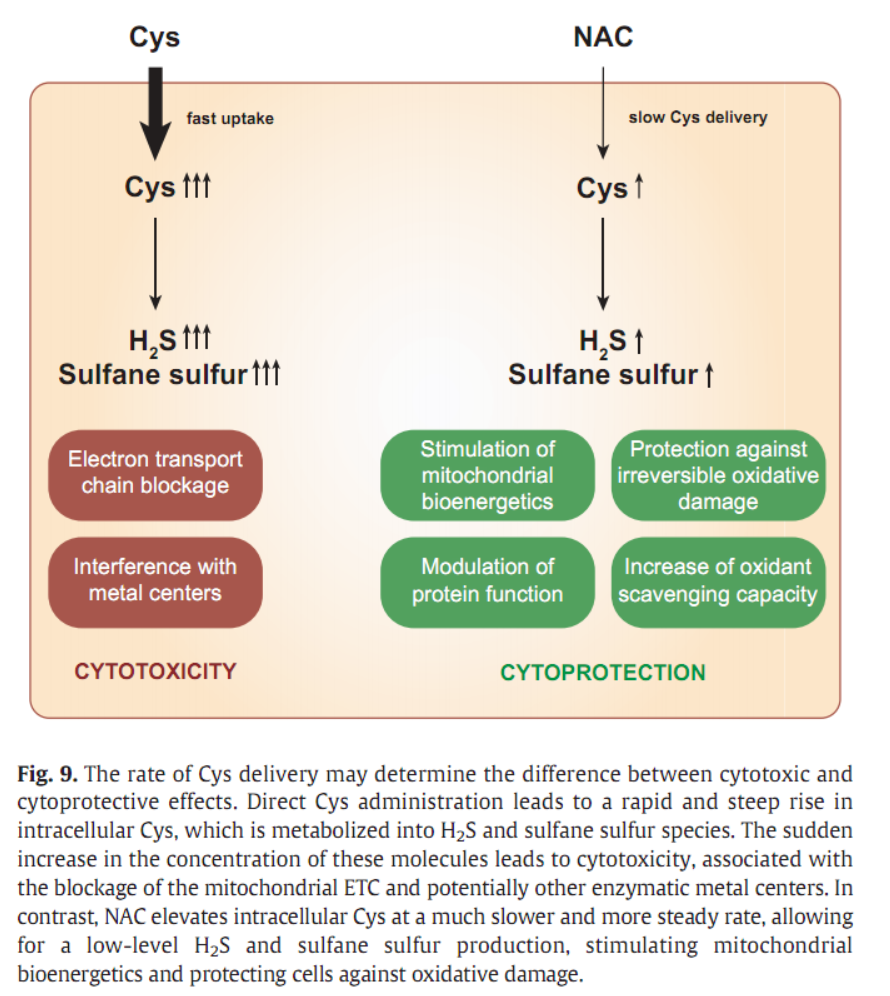
.Most likely, uptake rather than deacetylation is the rate-limiting step, as a more lipophilic NAC derivative, NAC ethyl ester, shows enhanced intracellular Cys delivery relative to NACFrom The mechanism of action of N-acetylcysteine (NAC): The emerging role of H2S and sulfane sulfur species you get these illustrations:
Also noteworthy:
Among the amino acids in protein, cysteine and cystine are well known to be among the poorest absorbed from the upper small intestine (NRC, 1994). Heat treatment of proteins contributes to the poor digestibility of cysteine because heating protein causes cysteine to be oxidized to cystine, a dimer that is poorly absorbed (Miller et al., 2001; Parsons et al., 1992)."
[Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate | Institute of the Medicines]acetylation of the amino group renders NAC resistant to oxidation, and even when it does get oxidized, ensures solubility of the oxidation product. This explains why NAC solutions do not precipitate over time, even after prolonged storage.
Noteworty especially regarding Coenzyme-A, which is not at all about B5-megadosing, and which also means that more acetaldehyde is allowed to be converted into acetic acid to be used for CoA:
"N‐acetylcysteine, which functions as a cysteine donor. Cysteine is critically important in energy metabolism by contributing the sulfhydryl (SH) group needed for energy generation. For example, coenzyme A (CoA‐SH) is an important component of reactions governing energy generation and depends on the availability of a SH group for its normal functioning."
Then there's a lot like the findings described therein (pigs are most similar to humans regarding GI systems):
N-Acetylcysteine improves intestinal function and attenuates intestinal autophagy in piglets challenged with β-conglycinin
and stuff likeTreatment with NAC significantly reversed the glucose intolerance, fasting glucose concentrations, and gains in body weight and plasma endotoxin in HFD-fed mice.
NAC upregulated occludin and mucin glycoprotein levels in the proximal colon of HFD-treated mice.
NAC promoted the growth of beneficial bacteria (i.e. Akkermansia, Bifidobacterium, Lactobacillus and Allobaculum) and decreased populations of diabetes-related genera, including Desulfovibrio and Blautia.and hints that it even epigenetically upregulates the CBS pathway:
Maternal NAC therapy prevented the rise in systolic blood pressure (BP) in male SHR [genetically altered Spontaneously Hypertensive Rats] offspring at 12 weeks of age. Renal cystathionine β-synthase (CBS) and 3-mercaptopyruvate sulphurtransferase (3MST) protein levels and H2S-releasing activity were increased in the SHR+NAC offspring. Maternal NAC therapy increased fecal H2S and thiosulfate levels in the SHR+NAC group. Additionally, maternal NAC therapy differentially shaped gut microbiota and caused a distinct enterotype in each group."
and other stuff like:
the study found the drug to be safe and effective at doses of 2.4 and 4.8 g/day in reversing the depletion of glutathione and in improving disease activity and the fatigue level."
[...] profoundly reduced mTOR activity in T lymphocytes
[...] kynurenine’s accumulation plays a role in the activation of mTOR in SLE
[...] Treatment with NAC increased the abundance of NADPH which in turn resulted in increased catabolism by NADPH-dependent kynurenine hydroxylase leading to lower levels of kynurenine which subsequently inhibited the mTOR pathway in those T cells
[...] A higher-than normal mitochondrial transmembrane potential or mitochondrial hyperpolarization (MHP) was found in lymphocytes from SLE patients.
MHP is attributed the blocked electron transport, and it is associated with the depletion of ATP and glutathione and the accumulation of oxidative stress-generating mitochondria due to diminished mitophagy.
"Kynurenine accumulation has been reversed by treatment with NAC but not placebo in the setting of a double-blind placebo-controlled clinical trial of 3-month duration."
oral administration is reported to lead to NAC concentrations below 15 μM in the circulation whereas intravenous injections of NAC achieve serum concentrations between 100 and 1500 μMOrally, it undergoes rapid intestinal absorption and metabolism by the liver, which directs most of the cysteine released toward GSH synthesis.
Intravenous administration allows rapid delivery of high concentrations of NAC due to the absence of the first-pass intestinal and hepatic metabolism and that is why it is the intravenous route used for the treatment of paracetamol overdose
For oral administration, this seems to be the predominant mechanism, with deacetylation taking place in intestinal enterocytes and Cys being forwarded through the portal vein, leading to a bioavailability of 9 and 4% for total and reduced NAC, respectively.
So only about 9% of oral NAC reaches circulation as NAC. The other 91% of oral NAC get taken up and deacelytated by enterocytes and hepatocytes.
GlyNAC supplementation for 24 weeks in Older Adults corrected RBC-GSH (glutathione) deficiency, oxidative stress, and mitochondrial dysfunction; and improved inflammation, endothelial dysfunction, insulin-resistance, genomic-damage, cognition, strength, gait-speed, and exercise capacity; and lowered body-fat and waist-circumference
Treatment with laxative or NAC reduced mucus accumulation by 43% and 50%, respectively, as measured histologically as dilation of the intestinal crypts. [...] Laxative and NAC also reduced bacterial overgrowth in the CF intestine by 92% and 63%, respectively.
NAC treatment reduced matrix metalloproteinase-2 (MMP-2) secretion and exhibited a direct effect on the secreted MMP-2 activity.
MMP-2 activity were restored to physiological value.
Compounds able to maintain GSH/GSSG ratio to physiological values can be useful to restore normal MMP-2 levels reducing in CD [Crohn's Disease] patient intestine the dysfunction of epithelial barrier.MMP-2 info for context:
(Matrix Metalloproteinase-2 (MMP-2) is a neutral, zinc-dependent protease that primarily targets extracellular matrix proteins It's dysregulation has been implicated in a variety of pathologies, including Alzheimer Disease.
.MMP-2 induces breakdown of BBB
.MMP-2 disrupts oxidative homeostasis
./MMP-2 has both proinflammatory/pro-angiogenetic and antiinflammatory/ anti-angiogenetic effectsNAC also restores neuroplasticity after cocain abuse (and from other stimulatory drugs), decreasing addiction and relapses:
N-acetylcysteine (NAC) treatment prevents relapse in animal models and craving in humans by activating cystine-glutamate exchange and thereby stimulating extrasynaptic metabotropic glutamate receptors (mGluR). NAC treatment of rats restored the ability to induce LTP and LTD by indirectly stimulating mGluR2/3 and mGluR5, respectively. Our findings show that cocaine self-administration induces metaplasticity that inhibits further induction of synaptic plasticity, and this impairment can be reversed by NAC, a drug that also prevents relapse.
Wherein LTP stands for Long-Term-Potentiation and LTD stands for Long-Term-Depression which has been found to induce brain cell apoptosis and elimination of synapses:
New evidence demonstrates there are similarities between the apoptotic pathway and LTD which involves the phosphorylation/activation of GSK3β. NMDAR-LTD(A) contributes to the elimination of excess synapses during development.
[MDMA] can lead to spatial memory impairments and hippocampal cell death
NAC significantly protected against MDMA-induced apoptosis and the up- and down-regulation of Bax and Bcl-2 [which are pro-apoptotic], respectively.
Attenuation of ecstasy-induced neurotoxicity by N-acetylcysteineNAC facilitates the release of dopamine (DA):
Dopamine itself is strongly prooxidant, forming hydrogen peroxide (H2O2) and free radicals through autooxidation and normal metabolism, and hence dysregulation of dopamine signalling is thought to be a major contributor to neurotoxicity [20].
[...] Methamphetamine evokes strong dopamine release and drives neuronal apoptosis.
[...] NAC ameliorates the oxidative stress induced by methamphetamine production and prevents the downregulation of the dopamine transporter elicited by excessive dopamine release.
[...] demonstrates the importance of cystine/glutamate transport and GSH regulation of oxidative stress in dopaminergic signalling
[The promise of N-acetylcysteine in neuropsychiatry. 10.1016/j.tips.2013.01.001, 2013]Noteworthy in the context of Peat's mentioned toxicity of (heterocyclic) biogenic amines by consumption of rotten aka "matured"/"aged"/"ripened" meat:
NAC N-acetylcysteine, alpha-tocopherol and glutathione were protective against N-hydroxylamine-mediated lactate dehydrogenase release into the medium.
N-acetylcysteine was by far the most protective of the agents investigatedIn summary, it seems that NAC delivers Cys at such a slow and (presumably) steady pace that it avoids the toxic effects that have been associated with corresponding dosages of unmodified Cys. In other words, N-acetylation of Cys slows down the delivery of Cys, making NAC a Cys-prodrug that feeds cells with a trickle of Cys over a prolonged period of time.
A new conceptual framework for NAC’s mechanism of action is emerging, namely as a Cys pro-drug that leads to modest elevations of H2S and sulfane sulfur species inside cells. The slow release of Cys from NAC allows for sustained sulfane sulfur production, providing protective effects -independently of GSH replenishment (Fig. 9). The sulfane sulfur branch of NAC metabolism opens new perspectives on its therapeutic use.It's important to consider though,
that NAC annihilates the antioxidant effects of lipoic acid in the NO-pathways on nerve cells, because LA exerts that effect through a mild pro-oxidant raise of Akt / decrease of GSK3-beta,
that NAC exerts anticoagulant and antiplatelet properties so would mess with bleeding disorders and blood thinning medications,
that all H2S-generating pathways require PLP/P5P as a cofactor so it's crucial to supply enough of this active vitamin B6,
that NAC hinders antibiotics, phagocytosis and pathogen elimination - unless its specifically Mtb against which it curiously assists,
that NAC (as well as e.g. melatonin) is a TLR4 antagonist and thus decreases beta-defensin expression of the innate immune system hence it's not a wise thing to take in acutely infected conditions and when tackling intestinal pathogens especially.@GRay I hope that helps you a little.
-
wow, that is amazing. thank you so much for putting this together, this should be a pinned post on NAC vs Cysteine
My anecdote:
Years ago I was having a gut issue, I started taking NAC slow released from Jarrow, and it literally improved the issue substantially in a matter of a day or two. -
@CrumblingCookie said in B-complex and or Multi recommendation?:
So only about 9% of oral NAC reaches circulation as NAC. The other 91% of oral NAC get taken up and deacelytated by enterocytes and hepatocytes.
@CrumblingCookie if I'm understanding well, even if most of the oral NAC is deacelytated, the cysteine will go mostly for GSH synthesis correct?, which seems to be a good thing, or this means it would be better not to take oral NAC because the deacelytated process?
did they use an oral or injection form in the studies you attached?
-
@GRay said in B-complex and or Multi recommendation?:
@CrumblingCookie if I'm understanding well, even if most of the oral NAC is deacelytated, the cysteine will go mostly for GSH synthesis correct?, which seems to be a good thing, or this means it would be better not to take oral NAC because the deacelytated process?
did they use an oral or injection form in the studies you attached?
You've got me thinking with your report on SR-NAC and your previous question, the answer to which appeared obvious only at first. It led me on and I had formulated extensive thoughts spinning off but didn't get a full grip on them and by now almost forgot what I wanted to say.
So yes it's curious that 300mg NAC i.v. will push tolerability to the limit, whereas grams of NAC p.o. are practically free of systemic side effects, with only roughly 10% reaching circulation as NAC and the other 90% being used up by the liver and intestine. GSH synthesis in the gut and liver would be a huge part of it, but the intracellular sulfation products too. The sulphur compounds are really important for intestinal and biliary mucus composition.
Which really made me wonder why NAC can be so "brutal" on digestion as in a very purgative sense: Naturally, the NAC dissolves the disulphid-bonds of mucus so it makes sense for it to break down not only biofilms but also the body's own mucin layers.
From there I pondered if a critical, minimum amount of NAC supplementation needs to be exceeded so that the single- or double-mucin-layered parts of the guts which are being eroded by NAC eventually get their fair re-supply of cysteine not from the GI lumen but through circulation. So that there needs to be "spare" NAC or cysteine to supply all necessary tissues beyond immediate needs of the liver etc.
What didn't quite add-up was the info that total GSH synthesis in an average adult is purported to be only about 2.3grams per day, whereof c. 900mg cysteine (@Amazoniac had written about that on the RPF). So c. 900mg L-cysteine per day = c. 1200mg NAC should about cover the whole body's GSH needs in an uninsulted basal state.Another aspect to why the purgative effect of NAC may only last a few days and then subside is that NAC not only dissolves biofilms but also turns out to be bacteriostatic and even bactericidal against common intestinal bacteria at practical concentrations of 500-1000mg per 100ml., so any brutal GI effects of NAC may simply require some days of patience or even an increase of dose or concentration.
I therefore went experimenting and found c. 3g supplemental NAC per day to be an effective optimum before it starts to give me a smoky and raspy voice. In that 2021 GlyNAC study in older adults they were given about 8g glycine and 10g NAC every day for almost 6 months.
Thanks go out to @Nokomi for valuably bringing L-threonine to my attention as a crucial element of mucin and mucin repletion.
From there on I've adapted my previous 1:1:1 NAC-Glycine-Glutamine blend to a 2:1:1:2 NAC-Glycine-Glutamine-Threonine blend, since a considerable part of the NAC is not going into GSH but into other sulphur compounds. So already by that, an equimolar glycine or glutamine ratio isn't needed.
The threonine can, in part, be converted to energy + glycine. It's thinkable to even forego the glycine completely and do 2:0:1:3. And eating any cereals will provide plenty of glutamine. But the 2:1:1:2 ratio seems to be a good, allround, working basis for both fed and fasting states in amounts of c. 2grs four times daily. That's 8grs per day, thereof 2.66grs NAC.
I'd say it's totally fine to take it twice as often or add several grams of extra threonine or at least take a good amount of whey or casein protein, which are well-balanced and contain much cysteine and threonine.I also compared taking NAC with taking potassium sulphate, thinking that lot of NAC will directly serve sulphation. However, IME, the KSO4 can only replace a small part of what the NAC does and I don't see benefits of doing more than 1-2g KSO4 per day. Sulphate seems tricky to me. Allegedly it's a difficult molecule to cross membranes and therefore may be mostly about increasing renal retention and an improved serum/intracellular SO4 gradient sparing some degree of catabolic intracellular protein breakdown to sulphate.
Elemental, anorganic sulphur did even less, with IME 0.5g twice daily already giving the beneficial maximum and declining at doses beyond that.Summing up, I find extra threonine crucial to go along with oral NAC. Lots of thoughts triggered by your follow-up question.
I can't allocate the forms of application to the bits of the various studies mentioned without a lot of tedious work. A lot of it was per os / orally.
-
@CrumblingCookie thanks for expressing your thoughts. I always learn allot from it!
Hello! It looks like you're interested in this conversation, but you don't have an account yet.
Getting fed up of having to scroll through the same posts each visit? When you register for an account, you'll always come back to exactly where you were before, and choose to be notified of new replies (either via email, or push notification). You'll also be able to save bookmarks and upvote posts to show your appreciation to other community members.
With your input, this post could be even better 💗
Register Login