@haidut said in Fish oil (omega-3) causes, not prevents cardiovascular disease (CVD):
using fish oil on a regular basis might actually increase the risk for healthy people to go on and develop first-time heart disease and stroke.”
Thank you for the highlighting and the source.
One question still remains unanswered.
Preamble
I am aware that it is necessary to avoid taking omega-3 supplements because they are easily altered, even if protected (…) and then thus contribute to the alteration of the oxidized membranes, especially when the support of tocopherols is absent (clearly insufficient via food). I take 500 IU from a 2x/week mix (Gamma E Complex, Now Foods). I read that the intake of vitamin E can saturate fat acids with long chains. (I didn’t find the source back, and this requires confirmation).
20 mg Vit for 10 gr of AGPI are required.
=>Ratio vitamin E / fatty acid in mg / g: 0.3/mono-; 2/di-; 3/tri-; 4/tetra-; 5/penta-; 6/hexaenoic fatty acid. (1-4)
Deduction: 10 gr omega-6 (ALA) needs 2 mg x 10 = 20 mg vit E.
Situation
The person regularly consumes less than 10 gr of PUFA per day, including 1.5 gr of ALA. He / I aim at 6 gr LA and 0.5 to 1 gr of omega-3. He also takes 0.2 gr from Vit C per day, 100 mcg Se 2x/ week. 2x/ week 500 UI of Toco (5) This person suffers from recurrent latent inflammation (backpain). He was doing a rotating with salicine, curcumin and Celadrin, for more than 15 years, without really taking a break, except when he was doing a water fast. (Not fine for the CYP450 evacuation pathway). But since this person did a treatment with vitamin B6 (100 mg PLP) (B1 B2 B3 B6 + TMG, according to a protocol and with pause), the pain manifests itself very rarely. B6 is also anti-inflammatory and moderates the immune response.
Question
Knowing that it would be appropriate to avoid adding a layer to the problem – oxidation of PUFA’s –, knowing that
the ratio and the amount AL / ALA is under control and at a moderate level (important), is it coherent / adequate to take half a tsp (2 gr) of oil rich in EPA, on a intermittent way,
well protected from oxidation (important).
Note that the protection time is only valid for 3 months, once the bottle is opened. After this period, I add an antioxidant (2 drops of Rosemary H.E.) (not vitamin E).
And once ingested, protection disappears. It must be renewed. (5)
I do this intermittently when I am between 6-10 gr of PUFA, without an adequate balance of omega-3 brought by food, only by food. I avoid oils, except olive oil and coconut. Omega-6 often comes from breakfast (Jordan oats + pecan nuts) 3x/week, and snack (wheat cake 2 x 24 gr or a Brownie 30 g). Note that there is an adequate SFA contribution at breakfast (Coco).
Sources et Références :
Efficacy of vitamin E in reducing oxidation of pufa
If 10 gr PUFA (1.5 W3 LA and 8.5 gr W6 ALA): (1.5 x 3) + (8.5 x 2) = 18.5 mg Vit E
Useful info:
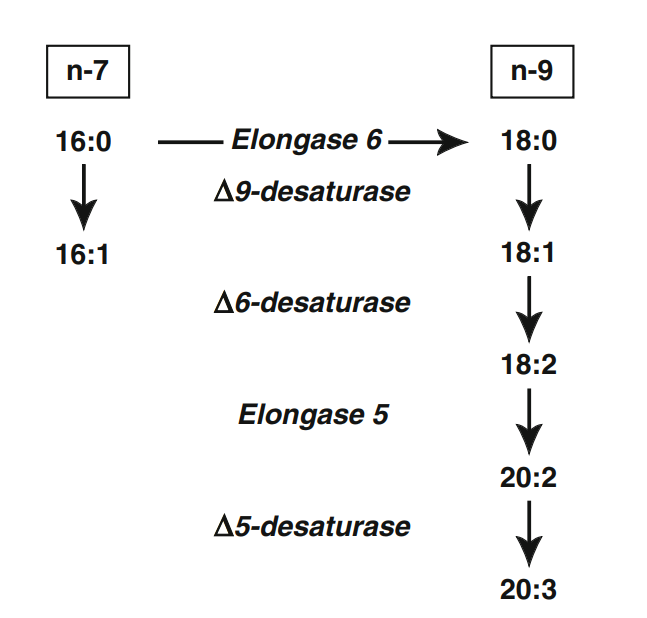
Mono-unsaturated fatty acid: Oleic acid. (Omega-9 = 9 Carbon atoms) 18:1 (9), n-9
Di-unsaturated fatty acid: Linoleic acid (LA / Omega-6). 18:2 (9,12), n-6 (2 doubles liaisons en n9 et n12 sur la chaine carbonée).
Tri-unsaturated fatty acids: Linolenic acid (ALA) (Omega-3). 18:3 (9,12,15), n-3 (3 doubles liaisons en n9, n12 et n15)
Tetra-unsaturated fatty acids: Arachidonic acid (AA). 20:4 (5,8,11,14), n-6 (4 doubles liaisons)
Penta-unsaturated fatty acids: Eicosapentaenoic acid (EPA). 20:5 (5,8,11,14,17), n-3 (5 doubles liaisons)
Hexa-unsaturated fatty acids: Cervonic acid (or docosahexaenoic acid). 22:6 (4,7,10,13,16,19), n-3
Note: Cervonic acid depends on consumption of omega 3 essential fatty acids (e.g., ALA or EPA), but the conversion process is inefficient. From fish oils.
Sources and references:
To be reminded 1:
“In declaring EPA and DHA to be safe, the FDA neglected to evaluate their antithyroid, immunosuppressive, lipid peroxidative (Song et al., 2000), light sensitizing, and antimitochondrial effects, their depression of glucose oxidation (Delarue et al., 2003), and their contribution to metastatic cancer (Klieveri, et al., 2000), lipofuscinosis and liver damage, among other problems.”
From “The great fish oil experiment”. Ray Peat PhD. 2007
http://raypeat.com/articles/articles/fishoil.shtml
*) To be reminded 2
Saturated Fat Protects Against Oxidation of Cholesterol Whereas Omega-6 Promotes It
When cholesterol is bound to saturated fat, it is protected from oxidation, which lowers your risk for cardiovascular disease, and when it is bound to linoleic acid, the cholesterol is susceptible to oxidation, thereby raising your risk.
The amount of linoleic acid contained in LDL can be seen as the true 'culprit' that initiates the process of oxidized LDL formation as it is the linoleic acid that is highly susceptible to oxidation.
Dietary linoleic acid, especially when consumed from refined omega-6 vegetable oils, gets incorporated into all blood lipoproteins (such as LDL, VLDL and HDL) increasing the susceptibility of all lipoproteins to oxidize and hence increases cardiovascular risk." 16
Vitamin E function and requirements in relation to PUFA
Daniel Raederstorff et al. Br J Nutr. 2015. doi: 10.1017/S000711451500272X
=>## 20 mg Vit E for 10 gr PUFA
*) The antioxidant function of vitamin E has been proven to be essential for preventing the oxidation of polyunsaturated fatty acids (PUFA) intake in men. PubMed 2000, E E Valk, G Hornstra – DOI: 10.1024/0300-9831.70.2.31
Vitamin E, Antioxidant and Nothing More
Maret G. Traber and Jeffrey Atkinson. 2007 doi: 10.1016/j.freeradbiomed.2007.03.024
The differences in potency of α-tocopherol versus other tocols in vivo is due to hepatic discrimination favoring α-tocopherol, as well as the preferential metabolism of non-α-tocopherol forms.
Excerpt:
Of the four tocopherols and four tocotrienols (designated as α-, β-, γ-, and δ-) found in food, only α-tocopherol meets human vitamin E requirements [15]. Despite the fact that all of these vitamin Es have similar antioxidant functions (rate constants for H-atom donation within an order of magnitude (Table)), non-α-tocopherols are poorly recognized by the hepatic α-tocopherol transfer protein (α-TTP) [16].
Quantitative Consideration of the Effect of Polyunsaturated Fatty Acid Content of the Diet Upon the Requirements for Vitamin E
https://doi.org/10.1093/ajcn/13.6.385 1963
Diets with E:PUFA ratios above 0.6 are predicted generally to protect against vitamin E deficiency, but diets with ratios lower than 0.6 are expected to have a depleting effect.
Synergy effect with vitamin E
“Vitamin C regenerates vitamin E and vitamin E protects β-carotene, helped in this by polyphenols. In the event of β-carotene supplementation (not advised: only 5-10 mg from food, note's editor), vitamin C regenerates vitamin E and β-carotene, and β-carotene seems to protect vitamin E without really explaining this phenomenon "(1)
Savings effect
Vitamin E is not just a vitamin. Vitamin C makes it possible to recycle oxidized vitamin E and thus prolong its lifespan. The same goes with glutathione which is thus saved for other more useful functions (detox). Glutathion is our antioxidant master. Vitamin E protects against the deleterious effects of polyunsaturated fatty acids when the latter are in excess. And it is quickly done!
John Libbey Eurotext - Anti-oxydants d’origine alimentaire : diversité, modes d’action anti-oxydante, interactions. Auteur : Claude Louis Léger.