@alfredoolivas Right, your realism about the matter is in the same spirit as my original post was in.
I also am not fully convinced that DHTE or DHTP is even necessary given that drostanolone, proviron, and transdermal testosterone all exist.
Dandruff or scalp irritation? Try BLOO.
@alfredoolivas Right, your realism about the matter is in the same spirit as my original post was in.
I also am not fully convinced that DHTE or DHTP is even necessary given that drostanolone, proviron, and transdermal testosterone all exist.
If someone wants to go full Walter White mode and attempt to add an ester, I'm all for it, but it requires a fume hood, solvents that are potentially hard to get, and some apparatus to purify the compounds at the various stages of the synthesis.
Unless someone is already involved in synthesizing drugs at home or has access to a lab, I wouldn't say this is exactly a walk in the park.
Fluorine is the most electronegative atom in the universe. So, the effect is probably because the fluorine atom makes the molecule metabolism resistant.
I think it stemmed from his view of the flow of energy as the most important phenomenon in the universe.
As the most energy-demanding organ, he often talked about evolution leading (in a quasai-aristotelian way) to the development of big-brained creatures.
So, he seemed to value the brain most highly of all, but not in a "digital" sense, but because it could resonate with the flux of energy in the universe.
With regard to the toxicity of the fluorine atom in Halotestin, I think the relevant question is: does the fluorine atom ever become unbound to the steroid molecule in the metabolism of Halotestin? If the answer is no, then I can't see how it could be "toxic" if fluorine is only toxic when it's in its ionic form.
At what doses of Proviron did you notice the slight anabolic/recomp effect?
Also, making DHTE or DHTP from base DHT is not "homebrewing" in the usual sense, that's organic chemistry synthesis.
It's not easy, and in order to convince yourself and anyone else for that matter that the final product did not contain the toxic solvents and catalysts you would have to use, you would need to do further analytic chemistry to confirm purity, which would likely involve LC/MS, or exact boiling point analysis, or some other advanced and highly expensive method.
You are correct. All cigarettes are required by law to contain flame retardants. You want to be inhaling flame retardants? BIG NO
They contain nicotine, which is converted to niacinamide in the body. Since niacinamide raises NAD+ levels, nicotine should too.
In fact, I found a study purporting to show just that.
Ya, that's right. Seldom in nature are there truly unique properties. If something exists, it's usually on a continuum that contains many other realities.
Ex. Coffee is not the only source of caffeine, rather, the methylxanthines are pervasive in nature.
Similarly, the indigestible "insoluble fibers" are pervasive.
Turnips probably have them too, just based on their similarity to carrots.
Maybe your body wants the NAD+ boost.
So maybe Niacinamide would work. Actually the combination of 250-500 mg niacinamide with 3-5 mg methylene blue should be really potent at increasing NAD+/NADH ratio.
So, if after doing that for a few days, you don't have the cravings, you might have satisfied a physiological desire.
On the other hand, you could try nicotine in its pure form. One company that make products with it is:
As I was using my old-school CASIO FX-300MS calculator, I realized that it was basically exactly what I was looking for. If only my desktop worked like it did.
I tested it out at, unsurprisingly, it has no backlight. The screen is invisible in the dark.
If only they could make desktops like the old handheld calculators. Would be extremely cool and retro.
Does your thyroid atrophy with those dosages?
Let's put the observation that caffeine doesn't increase testosterone in humans into context in light of the studies I shared about thyroid hormone (which shares caffeine's ability to increase cAMP).
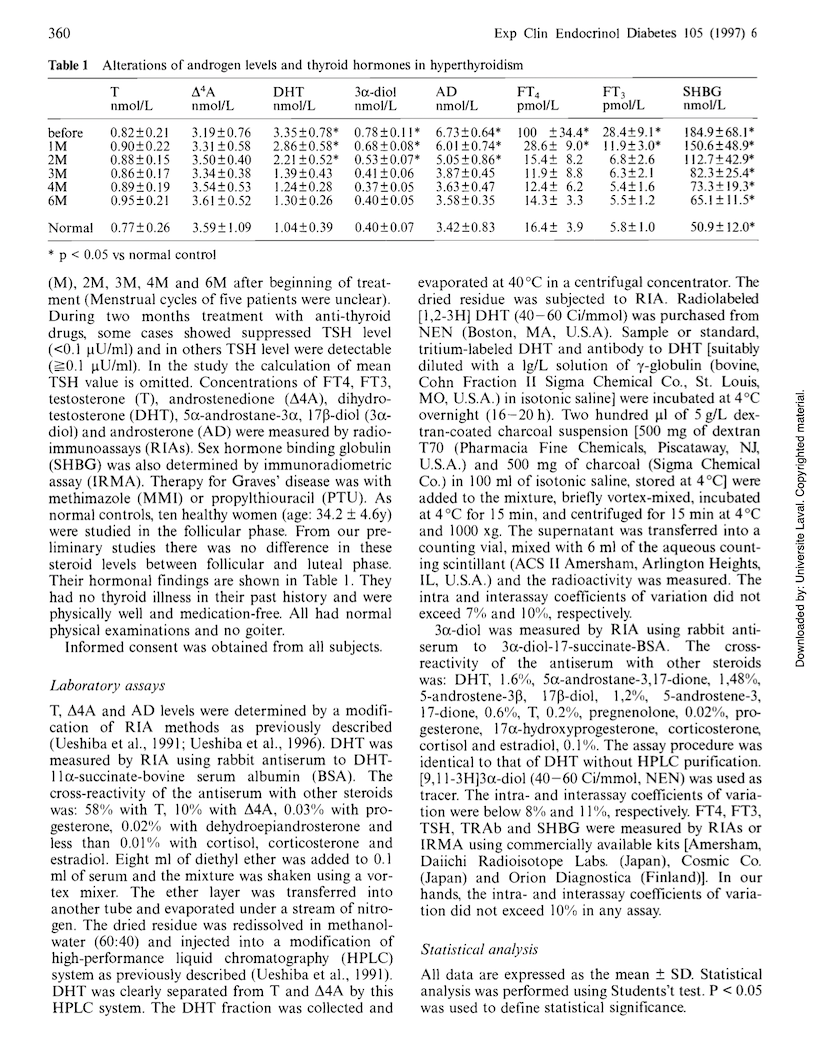
Recall that the hyperthyroid women did not produce significantly more testosterone than the normal thyroid women. In fact, at least at the 95% confidence level the study authors used, the amount of testosterone produced by the hyperthyroid women was not significantly different from that produced by normal thyroid women (0.82 nmol/L +- 0.21) vs (0.77 nmol/L +- 0.26), respectively.
Like I said, however, DHT difference absolutely was statistically significant. Hyperthyroid women had more than 3x DHT of normal thyroid women.
Androsterone and 5 alpha-androstane-3 alpha 17 beta-diol (androstanediol) were also significantly elevated.
Now, there are such things as the "backdoor" and "canonical" pathways of steroidogenesis.
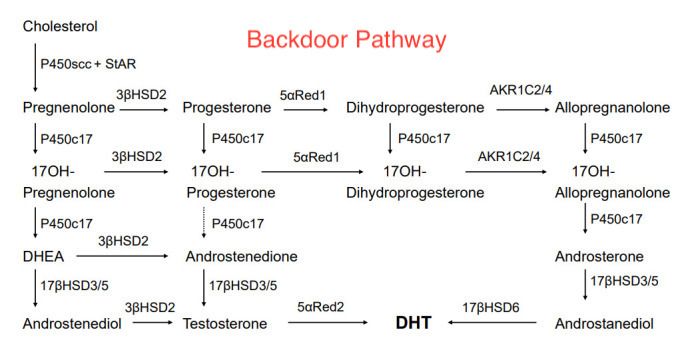
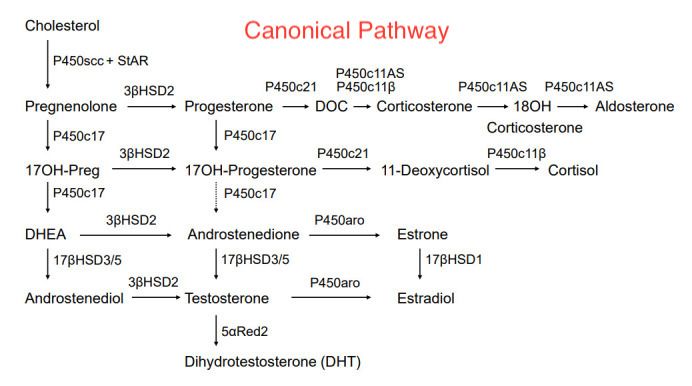
Since the study already admits that hyperthyroidism induces 5 alpha reductase, but testosterone levels were not elevated, and neither was androstenedione, this suggests that the backdoor pathway was being used.
And since androstanediol levels were high also, that suggests that 17 beta HSD 3/5 must also have been induced, for otherwise we would perhaps have expected elevated androsterone but not elevated androstanediol. Likewise 17 beta HSD 6 must have been induced as well to get elevated DHT from the elevated androstanediol.
So therefore the reason that androstenedione and testosterone were not elevated must have been because the progesterone and 17 hydroxy progesterone were mostly going toward dihydroprogesterone and 17 hydroxy-dihydroprogesterone from the induced 5 alpha reductase.
Therefore there were not significant enough amounts of those precursors available to make androstenedione and testosterone.
The difference between rats and humans with regard to caffeine intake is therefore probably due to rats and humans having different pathways for steroidogenesis.
In humans, we can tentatively say that caffeine favors the backdoor androgen synthesis pathway, which supports the idea that it increases the lipophilicity of cells as the backdoor pathway is more lipophilic than the canonical one.
Thank you for finding those studies. I'm actually going to use all of this in a separate thread I'll make sometime later that I think some forum members will find quite useful.
If caffeine does indeed increase the lipophilicity of the cell, then because we know that DHT (and I think also testosterone) induce the 5 alpha reductase enzyme, then just by entering the cell in higher abundance, these lipophilic androgens (especially DHT) should increase their own synthesis.
This is a positive feedback loop.
That caffeine increases cyclic adenosine monophosphate levels, which leads to more ATP and thus more cellular energy.
In fact, our friend t3 is thought to increase cellular metabolism in part to this same mechanism, by inhibiting phosphodiesterase, and increasing cAMP levels.
I was considering that as the mechanism by which it could cause cells to be more lipophilic.
[https://pubmed.ncbi.nlm.nih.gov/39626644/]
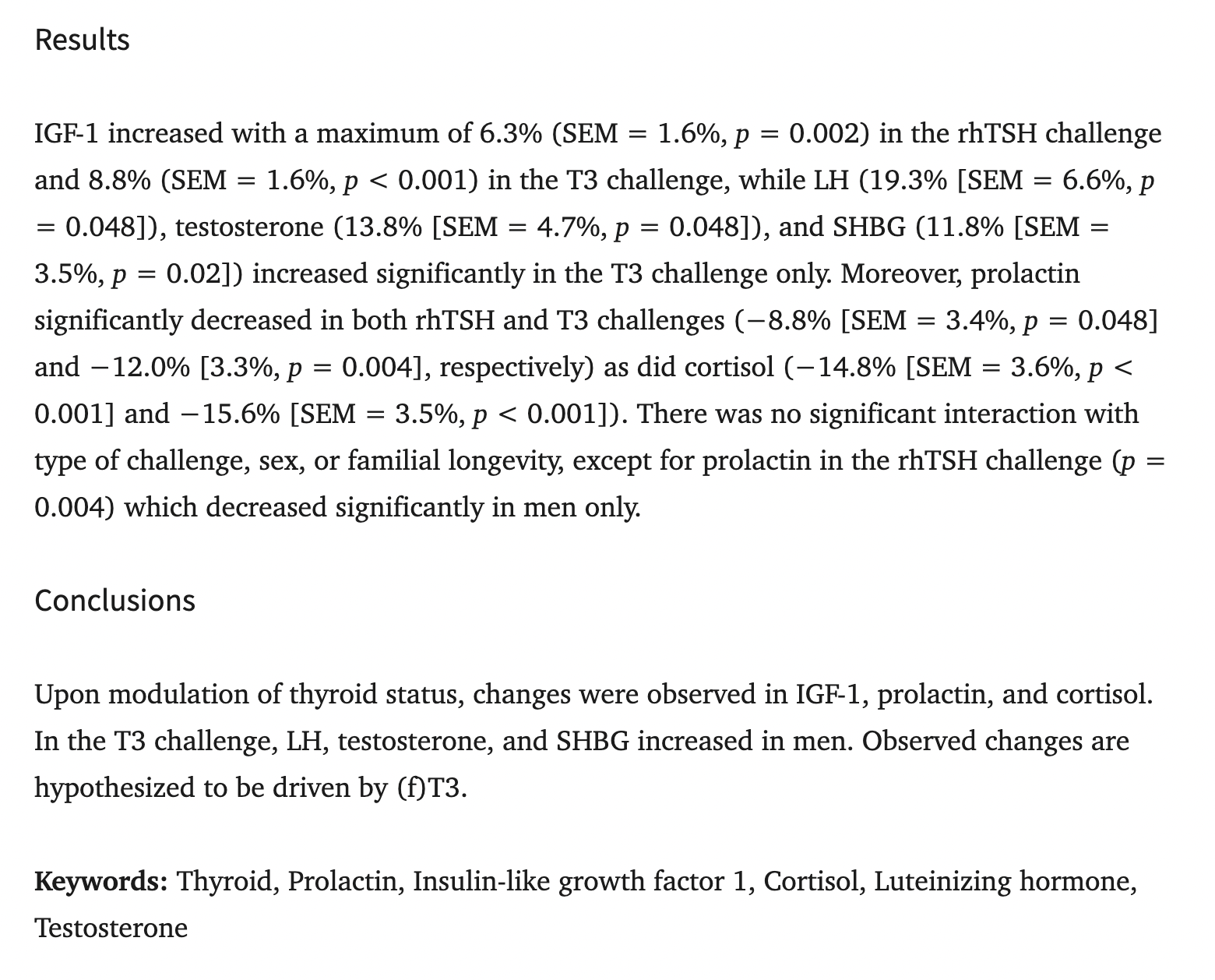
For example, it's known that t3 supplementation, even given to aging males at 100mcg orally, increases levels of testosterone by about 14% and decreases cortisol by about 16%
Now, I have another study showing that in hyperthyroid women (due to Graves' disease), Testosterone was slightly elevated, but, much more significantly, DHT was way higher.
In fact, in the untreated hyperthyroid women, DHT was about 3.3x the level of normal thyroid women and DHT/T ratio was more than triple that of normal thyroid women.
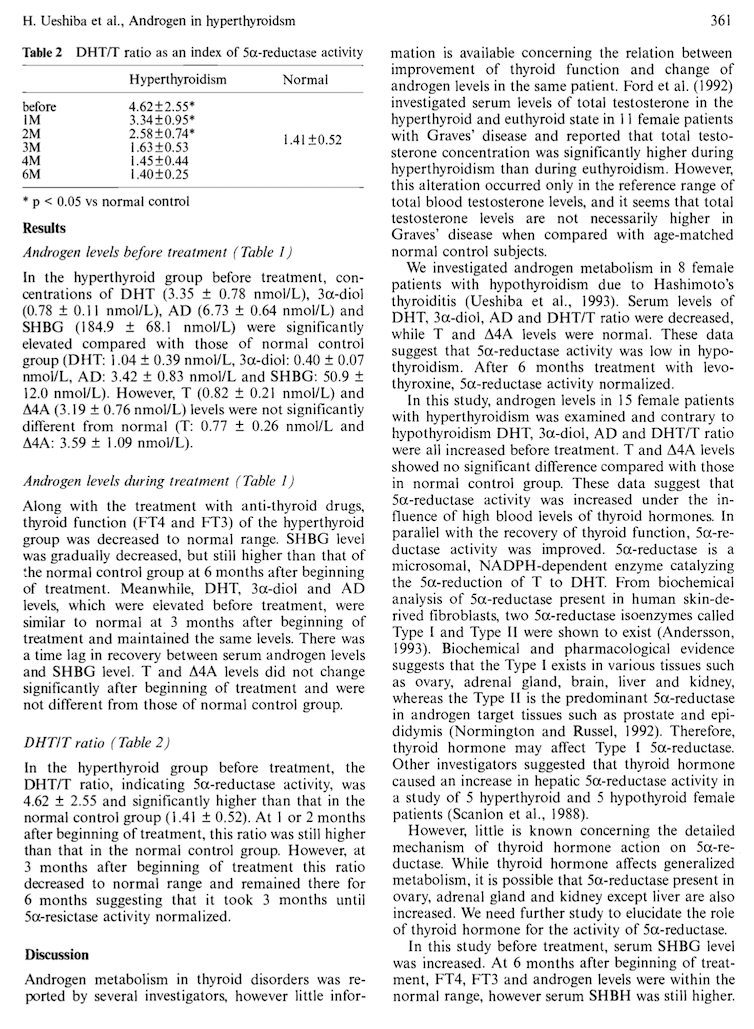
So, we see that when thyroid hormone is high (aka metabolism is high), cortisol decreases, testosterone increases, and DHT increases even more.
Well, it's almost as if t3 increases the synthesis of steroids in a way that is proportional to their lipophilicity ... remember the LogP values? Cortisol is much more hydrophilic, testosterone more lipophilic, DHT very lipophilic. So, it looks like t3 shifts the balance heavily toward more lipophilic steroids.
So, is it a stretch to say that the lipophilicity of the cell increases when metabolism is high? I don't think so.
So, I think it's plausible to say that anything that increases cAMP levels will increase the lipophilicity of the cell. Caffeine being an agent that does that, that explains why it increases the uptake of oxandrolone.
Well caffeine increases the expression of cAMP, which increases production of ATP, right? So maybe the effect is more global.
The way I was thinking about the effect of increasing the lipophilicity of the cell was that the cell would uptake more lipophilic steroids while excluding more hydrophilic steroids.
So, it would not be fully correct to say that a more lipophilic cell uptakes more steroids, rather it would uptake more lipophilic steroids, androgens among them.
So, if we look at the Log P values of the main steroids:
Estradiol (E2) – LogP ≈ 4.0
Progesterone – LogP ≈ 3.9
Dihydrotestosterone (DHT) – LogP ≈ 3.8
Testosterone – LogP ≈ 3.3
Androstenedione – LogP ≈ 3.0
11-Deoxycorticosterone – LogP ≈ 3.0
Androsterone – LogP ≈ 2.9
Dehydroepiandrosterone (DHEA) – LogP ≈ 2.8
11-Deoxycortisol – LogP ≈ 2.5
Estriol (E3) – LogP ≈ 2.5
Corticosterone – LogP ≈ 1.9
Cortisol (Hydrocortisone) – LogP ≈ 1.6
Aldosterone – LogP ≈ 0.5
As you can see, the mineralocorticoids and the main glucocorticoids are the least lipophilic, whereas the androgens and progesterone are more lipophilic.
The two caveats are that some of the glucocorticoids like 11-Deoxycorticosterone are more lipophilic, but it is actually well known that the more lipophilic a glucocorticoid is, the less it activates that glucocorticoid "receptor" and the more it behaves like progesterone or allopregnenalone.
In fact, the saturated cortisol derivative 5a,3a tetrahydrodeoxycorticosterone is actually a strong neurosteroid and ligand of GABA receptors, just like alloP and 3a-androstanediol
Also, estrogen is the most lipophilic of them all, however the other lipophilic steroids like DHT and progesterone that greatly outnumber it stop its synthesis and oppose its action.
So, the more lipophilic cell will be full of androgens, progesterone, more saturated and thus less catabolic glucocorticoids, and will exclude the mineralocorticoids and the catabolic glucocorticoids.
@Mauritio Whenever I go for a walk and see a pine tree or pine shrug, I pick of some of the needles, crush them between my fingers and smell it as I walk.
Probably the same effect.
Ya you gotta take everything with a grain of salt these days.
Ya, well, hyperthyroid people synthesize 4 times more androgens than hypothyroid people, so I guess I’ll choose doing things that move me closer to being hyperthyroid (enhancing glucose oxidation) than those things that move me closer to being hypothyroid (excess carnitine blocks glucose oxidation on multiple levels)