Pharmacological dosage of vitamin A as supplement
Inhibitors of retinol
We will assume that we are not dealing with vitamin A inhibitors. Mind when combining 2 or several factors: Alcohol (> 1 glass wine or beer a day), excessive coffee (more than 2-3 cups), cortisone, excess iron (>240; ideal ferritin level at 120 ng/ml), high amount of vegetable oils (> 5 g PUFA), smoking, anti-acid supplement, aspirin 500 mg without making staples (impact on platelets), …
Works synergistically with: Calcium, Phosphorus, Zinc, C, D, E*, Choline, Vitamin B* complex, EFA.
Too much of a good thing is bad.
Optimal range
There is no consensus about the ratio between HD A1 and D3.
Ratio 1:1 to 3:1 for retinol / Vit D3 is optimal when taking a supplement. For Chris Masterjohn
Ratio 4:1 to 8:1 for Dr. Lindsay. More vitamin A than vitamin D. In studies examining the protective effects of cod liver oil against upper respiratory tract infections, Dr. Lindsay and her colleagues used A-to-D ratios between 5:1 and 8:1.
Let’s say we should target 35 ng/mL 25(OH)D levels to limit immune problems. Target 45 ng is optimal
Chris Masterjohn has discussed the importance of maintaining a healthy balance between vitamins A and D, rather than focusing on high levels of either.
• 30 ng/mL as a minimum:
Many experts consider 25(OH)D levels of 30 ng/mL (75 nmol/L) and above to be sufficient for most adults to maintain bone health and potentially reduce the risk of some diseases.
• 40-60 ng/mL for potential benefits:
Some research suggests that higher levels within the 40-60 ng/mL (100-150 nmol/L) range may offer additional benefits, potentially reducing the risk of certain cancers, autoimmune diseases, and other conditions.
Note: When you reach a ceiling below 40 ng/mL Vit D, you must be careful not to exceed 420 mg of elemental magnesium. Has to be confirmed with practical guidance.
Optimal vitamin D level
There is some good evidence that 25(OH)D levels should be at least 30-35 ng/ mL (75-88 nmol/L). Much higher levels may be better, or they could start causing harm, especially in the absence of adequate vitamins A and K2. Once we leave the land of 30-35 ng/mL, however, we enter the land of speculation.
Sources:
Chris Masterjohn – Westonprice.org 2010.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8003866
Synergism between Vitamin A and Vitamin D but Excess Vitamin A causes Bone Problems
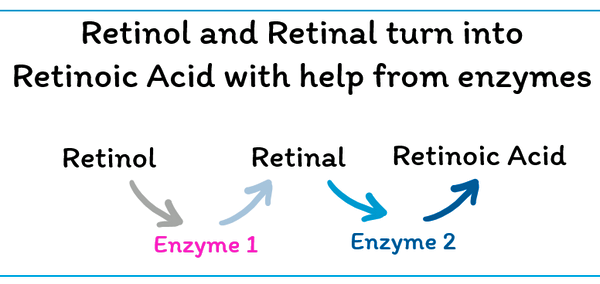
A study from NIH has shown that Vitamin A, specifically retinoic acid (RA), can increase Vitamin D Receptor (VDR) expression by up to 3-fold in certain cell types. This increase is observed in various tissues and cell types, including T cells and muscle cells, when treated with RA. The study also suggests that RA-induced VDR expression can be affected by Vitamin D, and vice versa, highlighting a complex interplay between these two important nutrients.
The dose from research was less than 5000 IU of Vitamin A (1500mcg) that get best benefits.
However, an increased VDR expression due to high level of retinoic acid (RA) can influence the downstream effects of both Vitamin A and Vitamin D signaling pathways.
doi: 10.3389/fimmu.2021.684015 Fatima A H Al-Jaberi et al. 2021. Front Immunol.
Interaction and Proposed Ratios
Chris Masterjohn describes a dynamic synergy: Vitamin A and vitamin D each mitigate the other’s toxicity, but when one is excessive relative to the other, metabolic harm may occur—such as bone loss (from too much A alone) or soft tissue calcification (from too much D alone). Vitamin K₂ is essential to activate key Gla proteins like osteocalcin and matrix Gla protein, helping ensure calcium goes into bone rather than soft tissues and articulations.
Source: mountaindogdiet.com interview with Chris Masterjohn: Dynamic synergy between vitamin A and vitamin D.
According to the gosling study (poultry nutrition), overly high A relative to D impaired growth—even moderate A antagonized D at low D levels. Growth was optimized with ratios closer to ~3.5:1 or lower.
Addressing Thyroid Status according to Ray Peat Considerations
I’ve noted Ray Peat’s concept of reducing retinoic acid when hypothyroid. In those cases, it may make sense to lean toward a lower A:D ratio, perhaps closer to 1:1, or even shift toward more D if RA synthesis slows. Evidence from community reports aligns: hypothyroid individuals frequently struggle to raise 25(OH)D even with doses alone, but see improvement when vitamin A is added—but only in appropriate ratios.
Thus, especially if hypothyroid, starting with ~1,000 IU A with ~1,000 IU D₃ may be more effective, slowly titrating both up while testing 25(OH)D serum, and watching for signs of imbalance.
Adressing the balance for liposoluble vitamins
Talk with ChatGPT. My final target (based on known data), making things reachable
• To reach 35 ng/mL 25(OH)D, ~2,000–3,000 IU D₃/day may be needed for most adults (see meta analysis: European adults ~2,500 IU/d → ~75 nmol/L, i.e. ~30 ng/mL) pubmed.ncbi.nlm.nih.gov.
• To maintain a sane A:D ratio between ~1:1 and 3:1, vitamin A intake at ~2,000–6,000 IU depending on your chosen D dose is reasonable.
• Your 1 mg K₂ MK 4 aligns well with vitamin K needs to activate the Gla proteins.
• Start perhaps with a mid point: 3,000 IU A in morning, 2,500 IU D₃ evening, and keep K₂ midday with fat. Check serum 25(OH)D and adjust.
Summary
Chris Masterjohn strongly advocates balanced A:D ratios (~1:1 to 3:1); 5:1 is higher than typical guidance and risks antagonism.
To reach 35 ng/mL D, I likely need 2,000–3,000 IU D daily.
Therefore 2,000–6,000 IU vitamin A, paired with your 1 mg MK‑4, would better align with balance principles.
And if hypothyroid, sticking closer to 1:1 may be safer.
All doses remain below toxicity thresholds (UL for A ≈ 10,000 IU/day; for D ≈ 4,000 IU/day) but we’re in pharmacologic range—monitor labs.
If you want more Vit A, start perhaps with a mid point: 3,000 IU A in morning, 2,500 IU D₃ evening, and keep K₂ midday with fat at 1 mg. Check serum 25(OH)D and adjust.
Supporting Chris Masterjohn Sources
• He emphasizes the necessity to balance A and D (synergistic moderation), and cautions that excess of one can poison the other’s benefits; optimal functioning requires balanced intake plus adequate K₂ to activate key proteins
• Balance extra 500 µg K₂ with 3,000 IU A and 900 IU D offers a template to scale up proportionally as doses rise.